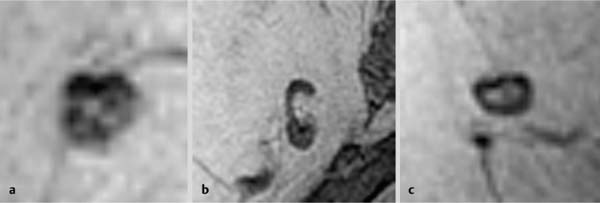
13 Lymph Node Diagnostics Lymphogenous spread of breast cancer is most commonly to the axillary lymph nodes. Rarely, breast cancer may also spread to the internal mammary lymph nodes or, even more rarely, to intraparenchymal lymph nodes. Good demarcation when in typical locations in subcutaneous fat tissue. Lobulated (Fig. 13.1a), oval (Fig. 13.1b), or bean-shaped (Fig. 13.1c), well-circumscribed, hypointense mass lesion. Lesions often display a central hyperintense area (fatty hilus) (Fig. 13.1). Rarely located within parenchyma, where the detection rate is reduced. Often a hyperintense mass (Fig. 13.2). When using a fat-suppressed sequence (e.g., IR sequence), a central signal-free zone is the correlate of the lipomatous lymph node hilus (Fig. 13.7b). Occasionally no or very little contrast enhancement within normal lymph nodes. Often reactive-inflammatory changes with increased peripheral perfusion (Figs. 13.4c, 13.5c, 13.6c). No perfusion of lymph node hilus (Fig. 13.5c). TIC usually shows intermediate or rapid initial signal increase and postinitial plateau or washout (Fig. 13.3d). Note: Lymph nodes with inflammatory changes and a fatty hilus may show findings resembling rim-enhancement (Fig. 13.3b,c). Lymph node locations. Axillary lymph nodes typically lie dorsal or lateral to the pectoral muscle (Fig. 13.4). Occasionally they lie in the prepectoral area (Fig. 13.3) or in the subcutaneous fat tissue lateral to the nipple (Fig. 13.5). Intramammary lymph nodes are typically found within the breast parenchyma (Figs. 13.6, 13.10, 13.11). Parasternal lymph nodes lie within the thorax along the internal mammary vessels (Figs. 13.12, 13.13). Lymph node size and morphology. The average diameter of typical, normal axillary lymph nodes is 5–10 mm. Lymph nodes with reactive-inflammatory changes, however, can easily reach diameters of 15–20 mm. Displacement or complete disappearance of a lymph nodes fatty hilus can be an indication of metastatic spread. A lymph node size over 15–20 mm (Fig. 13.9), or disappearance of the typical bean shape with an increasingly rounded shape (Figs. 13.8, 13.9) are indications of possible metastatic spread. The threshold values for parasternal lymph nodes is lower (Figs. 13.14, 13.15). a Round shape with lobulated borders. b Oval shape. c Bean shape.
 Breast imaging does not usually allow a reliable evaluation of metastatic tumor spread to local and regional lymph nodes.
Breast imaging does not usually allow a reliable evaluation of metastatic tumor spread to local and regional lymph nodes.
 MR Mammography: Lymph Nodes
MR Mammography: Lymph Nodes
T1-Weighted Sequence (Precontrast)
T2-Weighted Sequence
T1-Weighted Sequence (Contrast Enhanced)
 The size of axillary lymph nodes is reliably well visualized in the T1w and T2w images. Images after contrast administration are often of limited informative value in these areas due to overlapping of phase-encoding gradients.
The size of axillary lymph nodes is reliably well visualized in the T1w and T2w images. Images after contrast administration are often of limited informative value in these areas due to overlapping of phase-encoding gradients.
 The detection of a fatty hilus within a mass is almost always confirmation of a lymph node. It is not, however, proof that the lymph node is free of metastatic tumor spread (Fig. 13.7).
The detection of a fatty hilus within a mass is almost always confirmation of a lymph node. It is not, however, proof that the lymph node is free of metastatic tumor spread (Fig. 13.7).
Lymph Node Diagnostics
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


