 Apparent discrepancy: DCIS is an early diagnosis, but not always small.
Apparent discrepancy: DCIS is an early diagnosis, but not always small.Intraductal carcinomas: General information | |
Incidence: | Up to 20% of all breast carcinomas, depending on image quality. Comedo type accounts for 50% of all DCIS. |
Age peak: | 40–60 years. |
Multifocality: | ~30%. |
Bilaterality: | Not significantly increased. |
Risk of invasion: | Comedo type: ~50%. Noncomedo type: < 50%. |
Findings | |
Clinical: | Often clinically occult. Palpable mass in extensive cases (~10%). Rarely presents with pathologic secretion or mamillary changes (Paget disease). |
Mammography: | Suspicious microcalcifications (pleomorphic with linear, segmental, or clustered distribution). Rarely presents as architectural distortion or spiculated density. |
Ultrasonography: | Usually occult. Intraductal proliferations rarely display dorsal acoustic shadowing/extinction. |
Classification
Among other matters, the new WHO classification deals with current issues pertaining to traditional DCIS terminology and recommends additional use of the “ductal intraepithelial neoplasia” (DIN) classification system. The morphological variants of DCIS are divided into three main classes (DIN 1, DIN 2, DIN 3) and several subclasses.
The complete extent of a DCIS lesion is occasionally difficult to determine on breast imaging. The therapy of DCIS is still a subject of much debate.
 DCIS lesions are heterogeneous and considered to be precancerous lesions that can develop into invasive breast cancer. On the other hand, some DCIS lesions never become invasive. DCIS is a disease limited to the breast, not a systemic disease.
DCIS lesions are heterogeneous and considered to be precancerous lesions that can develop into invasive breast cancer. On the other hand, some DCIS lesions never become invasive. DCIS is a disease limited to the breast, not a systemic disease.
 MR Mammography: Intraductal Carcinoma
MR Mammography: Intraductal Carcinoma
T1-Weighted Sequence (Precontrast)
Normally there are no specific findings associated with DCIS because of its nonmass configuration (Figs. 11.2b, 11.6b, 11.9b). The spatial resolution of breast MRI is not sufficient for the visualization of microcalcifications. Rarely, DCIS may appear as a mass lesion (Figs. 11.4b, 11.11b).
T2-Weighted Sequence
No characteristic findings (Figs. 11.1c, 11.3c, 11.5c). Occasionally affected milk duct displays high signal intensity (Fig. 11.6c).
T1-Weighted Sequence (Contrast Enhanced)
Nonmasslike focal (Fig. 11.4a,d), linear (Fig. 11.1a,d), diffuse (Figs. 11.3a, d, 11.7a, c), rarely regional (Fig. 11.2a,d), frequently segmental (Figs. 11.6a, d, 11.8a, d, 11.12a, d) enhancement along the course of one or several milk ducts. Linear-branching enhancement pattern (Figs. 11.9a, d, 11.10a, d). Rare presentation as mass lesion (Fig. 11.11a,d), occasionally with rim-enhancement. TIC analysis of nonmasslike enhancement is of little value. Linear enhancement seen bordering on or near a suspicious mass lesion potentially represents an extensive intraductal component (EIC) (Fig. 11.13). Enhancing nodular areas within or in the periphery of a nonmasslike lesion potentially represents beginning tumor invasion, i.e., minimally invasive tumor stage (Fig. 11.14).
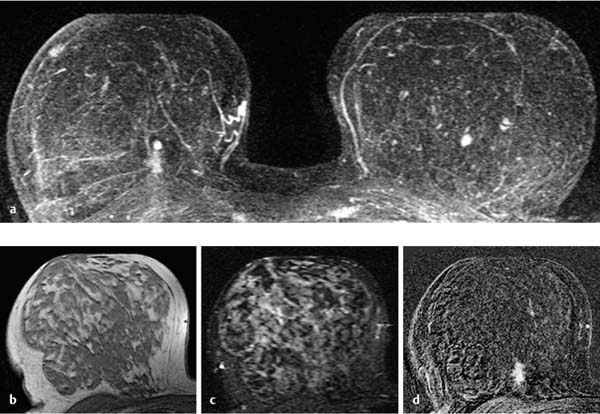
Fig. 11.1a–d Low-grade DCIS, linear.
a Subtraction MIP: a broad linear enhancing area is projected dorsally of a fibroadenoma in the right breast. Coincidental fibroadenoma in the left breast.
b T1w precontrast slice image (right breast): unremarkable findings.
c IR T2w slice image (right breast): unremarkable findings.
d Early subtraction slice image (right breast): better visualization of ill-defined, linear enhancement.
Histology: DCIS, grade 1.



