93 Infections of the Urinary Tract
Etiology and Pathogenesis
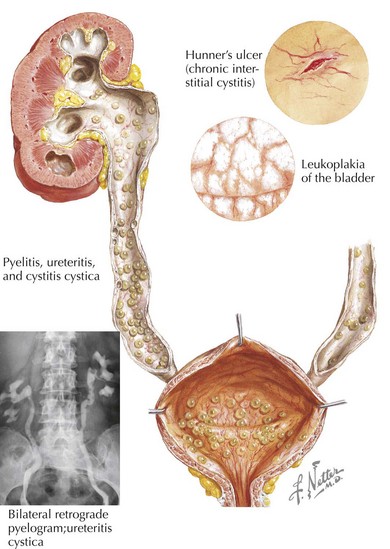
Infections of the urinary tract begin with ascension of flora that transiently colonize the lower urinary tract. The most common organism responsible for infection is the enteric gram-negative organism Escherichia coli. Other gram-negative organisms include Klebsiella, Proteus, Citrobacter, and Enterobacter spp. Gram-positive infections by enterococcus, Staphylococcus saprophyticus, and rarely Staphylococcus aureus are also known to occur. For infection to take place, the organisms must not only be present in the urinary tract but also needs to attach, adhere to, and invade the mucosa and epithelium. The bacteria are then able to ascend via the epithelial cells to the bladder and kidney (Figure 93-1). It is thought that genetically determined variation in the host’s defense against this process may explain the familial association of UTIs among first-degree relatives.
Clinical Presentation
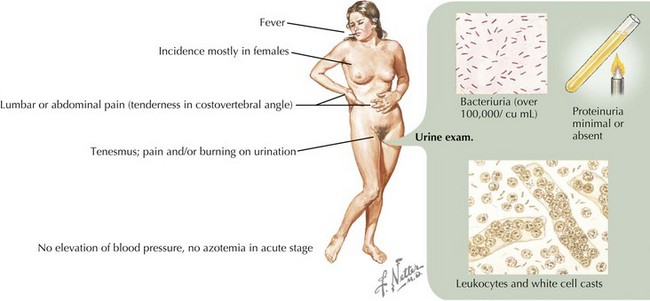
On physical examination of an infant or child with suspected UTI, it is important to note the degree of fever (if present) and any signs of cardiovascular instability that would reflect severe illness. Other findings on examination, more common in older patients, may include suprapubic or costovertebral tenderness. A complete abdominal examination should be performed to assess for any abdominal masses or abnormal distension of the bladder. A genital examination should look for any signs of urethritis or vulvovaginitis and for any anatomic abnormalities. If the patient is febrile, attention should also be paid to other potential sources of fever (Figure 93-2).