CHAPTER 21 Imperforate Anus
Step 1: Surgical Anatomy
♦ Anorectal malformations occur in 1 in 4000 neonates and are found slightly more commonly in boys than in girls. The most common defects in girls are rectovestibular fistula followed by perineal fistula and persistent cloaca. The most common in boys is a rectourethral fistula followed by perineal fistula. Rectobladder neck fistulas in boys occur in 10% of patients, and imperforate anus without fistula in both boys and girls represents only 5% of the entire group of defects.
Step 2: Preoperative Considerations
Associated Defects
Sacrum and Spine
♦ The sacrum is often abnormal, and the degree of sacral development correlates with the quality of sphincter and nerves and thus the final functional prognosis.
♦ Traditionally the number of vertebrae was the criterion for evaluating the sacrum. One missing vertebra does not have important diagnostic implications. More than two absent vertebrae represent a poor prognostic sign.
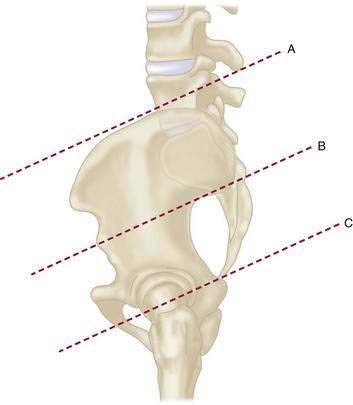
♦ To improve the prognostic accuracy based on sacral abnormalities, a sacral ratio was created that expresses the degree of sacral development. For this measurement, three lines are drawn: line A extends across the uppermost portion of the iliac crests; line B joins both inferior and posterior iliac spines; and line C runs parallel to lines A and B and passes through the lowest radiologically visible sacral point. In normal children the ratio of the distances BC:AB is between 0.7 and 0.8 in both anteroposterior and lateral projections (Fig. 21-1). Children with anorectal malformations suffer from different degrees of sacral hypodevelopment, with the ratio varying between 0 and 0.8. A ratio of less than 0.4 usually signifies a poor functional prognosis.
Urogenital Defects
♦ The frequency of associated urogenital defects varies from 25% to 50%. Patients with persistent cloaca or rectobladder neck fistulas have a 90% chance of having a significant associated urologic abnormality; infants with minor defects (perineal fistula) have a less than a 10% chance.
♦ The most common urologic malformation associated with imperforate anus is absent kidney, followed by vesicoureteric reflux. Hydronephrosis, urosepsis, and metabolic acidosis from poor renal function represent the main sources of mortality in neonates with anorectal malformations.
Management of Anorectal Malformations During the Neonatal Period
♦ Two important questions must be answered during the first 24 hours of life: what are the associated anomalies, and what operation is required—a newborn pull-through or a colostomy?
Males
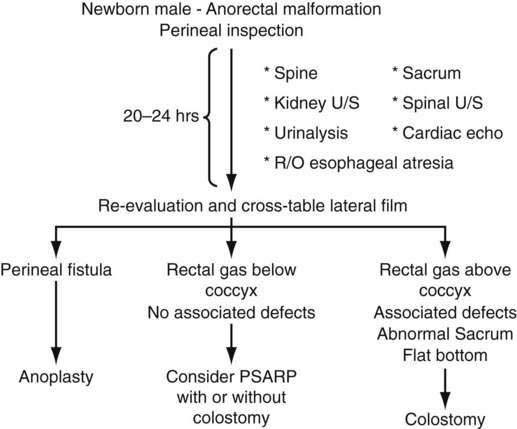
♦ The decision-making algorithm for the management of male newborns with anorectal malformations is shown in Fig. 21-2.
♦ Associated malformations must be investigated. In more than 80% of boys, perineal inspection and urinalysis provide enough information to make a clinical diagnosis. If a perineal fistula exists, the patient may be treated with a minimal posterior sagittal anorectoplasty. The presence of a flat bottom and meconium in the urine are indications for a diverting colostomy. The colostomy decompresses the intestine in the neonatal period, provides access for a contrast study to define the anorectal anatomy, and will subsequently provide protection against infection during the healing process after the definitive repair.
♦ It is important to wait 20 to 24 hours before deciding what operation to do. These patients do not show abdominal distention during the first few hours of life, and even if a perineal fistula is present, meconium is not usually seen on the perineum until 20 to 24 hours after birth. Radiologic evaluations are inaccurate because of the presence of meconium in the blind pouch of the intestine, interfering with the migration of air into the pouch and giving a false image of a high defect. A significant amount of intraluminal rectal pressure is required to reach a level high enough to overcome the voluntary muscle tone that keeps the most distal part of the rectum compressed.
♦ Shortly after birth, intravenous fluids are administered and a nasogastric tube is inserted to keep the stomach decompressed, thus avoiding the risk of vomiting and aspiration. Antibiotics are administered, and an ultrasound study of the abdomen is performed to rule out the presence of other anomalies (mainly urologic). A piece of gauze is placed on the tip of the penis, and the nurses are instructed to check for particles of meconium on this gauze.
♦ If after 20 to 24 hours of observation there is no clinical evidence indicating the need for a colostomy or a perineal operation, the patient should have a cross-table lateral film with the patient in the prone position to determine the position of the rectal pouch. The anal dimple is marked. If the rectum is visible below the coccyx, the patient can undergo a primary newborn repair, provided the surgeon is experienced with this technique. If the image is questionable, it is preferable to perform a diverting colostomy.
♦ The patient is discharged to home after recovery from colostomy placement. If the patient is growing well and has no other associated defects (cardiovascular or gastrointestinal) that require treatment, he is readmitted at 6 to 12 weeks of age for a posterior sagittal anorectoplasty after undergoing a distal colostogram. This early repair can be performed safely only if the surgeon has experience in dealing with the delicate anatomy of the infant.
♦ Performing the definitive repair early in life has important advantages for the patient, including less time with an abdominal stoma, less size discrepancy between proximal and distal stomas at the time of colostomy closure, simpler anal dilatation, and no recognizable psychological sequelae from painful perineal maneuvers. In addition, at least theoretically, placing the rectum in the right location early in life may represent an advantage in terms of acquired local sensation.
♦ Some surgeons have proposed primary repair of all anorectal malformations during the neonatal period without a protective colostomy. There is no question that this can be done and that it has the potential of avoiding the morbidity related to the formation and closure of a colostomy. The disadvantages include the fact that the tissue planes of the neonate are not as well defined as in older patients. Also, the diagnostic tests used to determine the level of the defect are not accurate enough, and the surgeon is actually subjecting the patient to a blind exploration of the perineum. If the rectum is located high in the abdomen, the surgeon may damage other structures during the search for the rectum. Such structures include the posterior urethra, seminal vesicles, vas deferens, bladder neck, and ectopic ureters. In addition, there is a risk of dehiscence and infection because the stool is not diverted.
Females
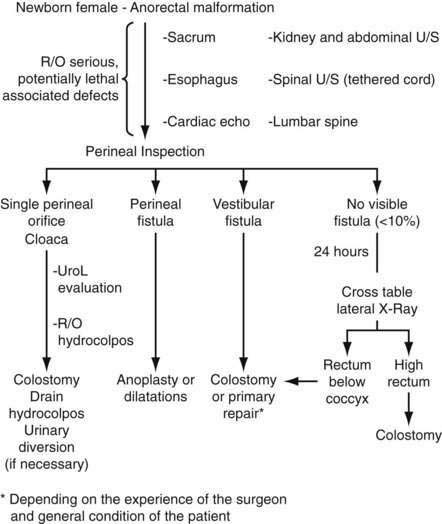
♦ A decision-making algorithm for the initial management of females is shown in Fig. 21-3. Perineal inspection usually provides more information in girls than in boys. The principle of waiting 20 to 24 hours before making a decision is again valuable.
♦ The presence of a single perineal orifice is pathognomonic for a cloaca. Because of their complexity, these defects are dealt with in a separate chapter.
♦ Perineal inspection may reveal the presence of a vestibular fistula (Fig. 21-4, in prone position), which is the most common condition in girls. In cases with rectovestibular fistula, the rectal orifice is located within the vestibule and outside the hymen. A true rectovaginal fistula is an extremely rare anomaly.
♦ These patients can undergo a primary repair via a posterior sagittal approach, either in the newborn period or following a period of dilatations, provided that the surgeon has adequate experience and that a meticulous technique is used. Our preference is to perform the repair during the newborn period. A colostomy followed by the definitive repair is an acceptable and safe approach. These fistulas are usually large enough to decompress the gastrointestinal tract. Occasionally the fistula is too narrow, and the patient will suffer from abdominal distention. In these patients the fistula may first be dilated to facilitate emptying the rectum. The defect is then repaired with a limited posterior sagittal operation.
♦ Patients with vestibular fistula are the ones most often referred after a failed attempt at a primary repair without a colostomy. Patients with vestibular fistula are usually continent after a successful operation. Infection or dehiscence may damage the continence mechanism and change the final functional prognosis.
♦ The presence of a rectoperineal (cutaneous) fistula is the simplest defect in the spectrum of female malformations. These patients can be treated with a minimal posterior sagittal anoplasty without a colostomy during the neonatal period.
♦ Most girls with imperforate anus (95%) have a fistula. Sometimes, after 20 to 24 hours of observation, the neonate’s abdomen may become distended without any evidence of meconium passing through the genitalia. In such a case, the infant probably has imperforate anus without fistula. The neonate should have a cross-table lateral film as described previously.

High-Pressure Distal Colostography
♦ Before the definitive repair, distal colostography is performed. It is the most valuable and accurate diagnostic study for anorectal malformations. Water-soluble contrast medium is instilled into the distal stoma, which fills the distal intestine and enables demonstration of the location of the blind rectum and the precise location of a rectourinary fistula. The rectum is surrounded by striated muscle, which keeps it collapsed and prevents filling of its most distal part. This may give the erroneous impression of a very high defect and may prevent demonstration of a rectourinary fistula. To avoid this problem, the contrast medium must be injected with hydrostatic pressure under fluoroscopic control. The use of a Foley catheter is recommended; it is passed through the distal stoma, the balloon is inflated (2 to 5 mL), and it is pulled back as far as possible to occlude the stoma during the injection of the contrast medium. This maneuver permits exertion of enough hydrostatic pressure (syringe manual injection) to overcome the muscle tone of the striated muscle mechanism, fill the rectum, and demonstrate the urinary fistula when present.
♦ In cases of rectourethral fistula (prostatic and bulbar), the surgeon will know preoperatively precisely where to find the rectum. In cases of rectobladder neck fistulas, the surgeon will not expect to find the rectum through the posterior sagittal approach and so avoids a blind perineal dissection. In this latter case, the surgeon can prepare the patient for an additional laparoscopy or laparotomy to mobilize a very high rectum.
Step 3: Operative Steps
Males
Perineal (Cutaneous) Fistula
♦ This type of defect is also known as a low imperforate anus. The rectum is located within most of the sphincter mechanism, but only the lowest part is anteriorly displaced.
♦ Sometimes the fistula follows a subepithelial midline tract opening along the midline perineal raphe, scrotum, or penis. The perineal findings in this kind of defect include a prominent skin tag, below which an instrument can be passed, known as a “bucket-handle” malformation (Fig. 21-5, in prone position), a black or white, ribbon-like, midline structure that represents a subepithelial fistula filled with meconium or mucus or a very well-formed anal dimple suggesting the presence of a very low defect. The diagnosis is established by perineal inspection. No further investigations are required.

Rectourethral Fistula
♦ This is the most common defect in boys. The rectum may communicate with the lower part of the urethra (bulbar urethra) (Fig. 21-6) or with the upper urethra (prostatic urethra). Immediately above the fistula site, the rectum and urethra share a common wall with no plane of dissection.
♦ This anatomic fact has important technical and surgical implications. The rectum is surrounded laterally and posteriorly by the levator muscle mechanism. Between the end of the rectum and the perineal skin, there is a portion of striated voluntary muscle called the muscle complex




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
