47 Hypertension
Etiology And Pathogenesis
Definitions
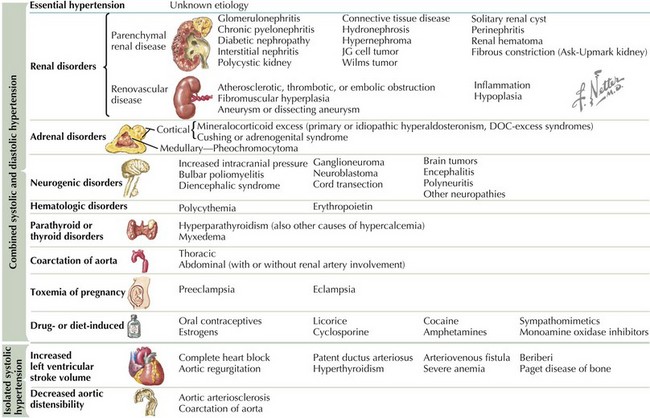
There are many causes of hypertension (Figure 47-1). Whereas BP for which a clear cause can be determined is described as secondary hypertension, hypertension without a clear correctable cause is referred to as primary or essential hypertension. This is necessarily a diagnosis of exclusion.


Clinical Presentation
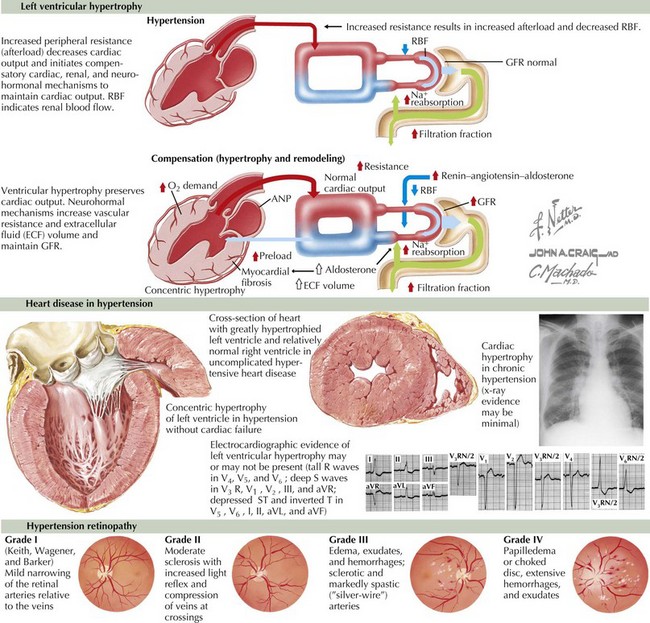
Most children with hypertension have not had years of exposure to elevated BPs. Therefore, unlike their adult counterparts, the clinical signs and symptoms in children and adolescents are generally more indicative of the cause of their disease rather than stigmata of end-organ damage from chronic hypertension. Although hypertensive nephropathy, left ventricular hypertrophy, congestive heart failure, hypertensive retinopathy, and stroke can be seen in children with long-standing, severe hypertension, they are much less common than in adults with chronic hypertension (Figure 47-2).
Evaluation
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


