100 Hyperbilirubinemia
Etiology and Pathogenesis
Because of multiple different etiologies, some infants develop more severe hyperbilirubinemia. Increased bilirubin production can occur in infants with increased RBC breakdown (G6PD [glucose-6-phosphate dehydrogenase] deficiency, ABO incompatibility, cephalohematoma) or elevated total body RBC stores (polycythemia, infants of diabetic mothers). Decreased bilirubin conjugation also contributes to hyperbilirubinemia in some infants because of decreased activity of UDPGT in Crigler-Najjar and Gilbert’s syndromes. Additionally, breastfeeding jaundice can occur early in the neonatal period in the setting of poor breast milk supply and associated dehydration and decreased stool output in an exclusively breastfed infant. In contrast, breast milk jaundice usually peaks during the second week of life and may take several more weeks to resolve completely. The mechanism of this process is not entirely understood but may involve components of breast milk inhibiting hepatic conjugating enzymes or increasing enterohepatic circulation. All of the aforementioned processes, because of their position in the bilirubin pathway, cause unconjugated hyperbilirubinemia (Box 100-1 and Figure 100-1).
Box 100-1 Selected Differential Diagnosis of Unconjugated and Conjugated Hyperbilirubinemia
| Unconjugated Hyperbilirubinemia | Conjugated Hyperbilirubinemia |
|---|---|
G6PD, glucose-6-phosphate dehydrogenase; IDM, infant of a diabetic mother; TORCH, toxoplasmosis or Toxoplasma gondii, other infections, rubella, cytomegalovirus, and herpes simplex virus; UTI, urinary tract infection.
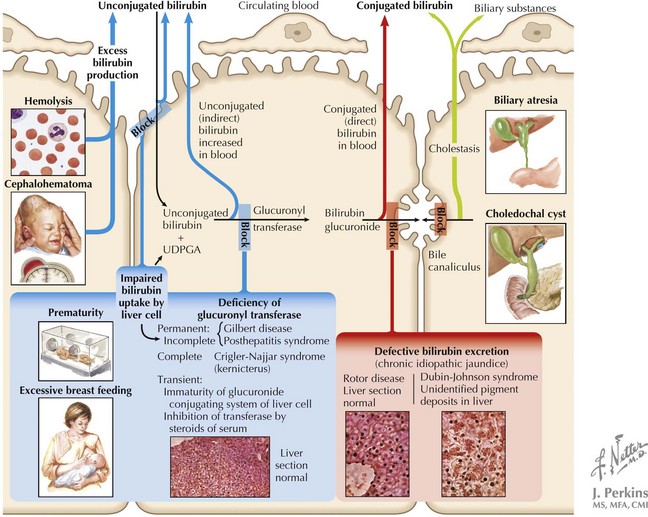
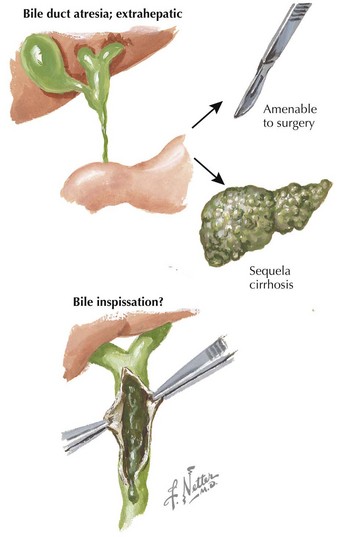
Conjugated hyperbilirubinemia occurs when the defective step exists after the conjugation of bilirubin, specifically involving defects in bile flow resulting in neonatal cholestasis (see Figure 100-1). The differential diagnosis of neonatal cholestasis is vast, including structural anomalies such as biliary atresia, choledochal cysts, and Alagille syndrome, metabolic disorders, including α-1 antitrypsin deficiency, galactosemia, and tyrosinemia, and endocrinopathies such as hypothyroidism (Figure 100-2). Additionally, infectious causes include viral (cytomegalovirus, HIV, herpes simplex virus), and bacterial (sepsis, urinary tract infections), and parasitic infections have been associated with conjugated hyperbilirubinemia. Other causes of conjugated hyperbilirubinemia include inherited deficiencies in excretion (Dubin-Johnson and Rotor’s syndromes), chromosomal disorders, parenteral nutrition, vascular and neoplastic processes, and idiopathic neonatal hepatitis (see Box 100-1).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


