Fig. 1
Indirect inguinal hernia. The indirect inguinal hernia passes first through the internal inguinal ring and then through the external inguinal ring after traversing the inguinal canal (Source: National Digestive Diseases Information Clearinghouse, National Institutes of Health, Bethesda, MD. http://digestive.niddk.nih.gov/ddiseases/pubs/dictionary/e-k.aspx. Downloaded 22 Dec 2013)
(ii)
Direct hernia: Represents a defect within the inguinal floor (transversalis fascia), medial to the epigastric vessels.
(iii)
Femoral hernia: Also represent a defect in the posterior inguinal floor. The hernia passes thru the femoral ring deep to the inguinal ligament and emerges within the femoral canal at the fossa ovalis.
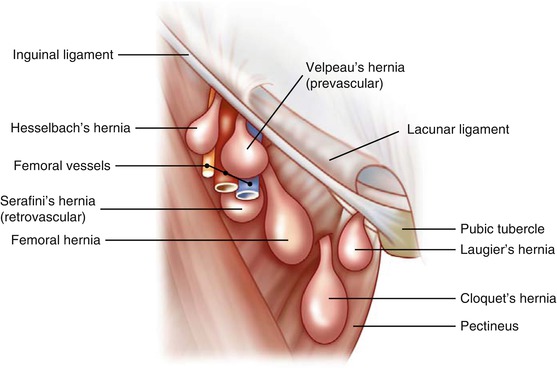
Fig. 2
Femoral hernia types. Femoral hernias are defects in the abdominal wall between the inguinal ligament and the upper pubic ramus (Source: Dr. Kumar Nishant, under Creative Commons Attribution Share-Alike 3.0 Unported license, from https://upload.wikimedia.org/wikipedia/commons/6/6e/Femoral_hernia_types.jpg. Downloaded 22 Dec 2013)
{kind=link}
(iv)
Sliding hernia: Any hernia of which a portion of the sac contains viscera.
(v)
Incarcerated hernia: Any hernia in which a portion of viscera is lodged and represents a surgical urgency.
(vi)
Strangulated hernia: Any hernia in which an incarcerated portion of viscera has lost its blood supply and represents a surgical emergency.
(b)
Anatomy:
(i)
Fascial layers of the abdominal wall contribute to layers of the testis and spermatic cord during testicular descent.
1.
Transversalis fascia → internal spermatic fascia.
2.
Internal oblique → cremaster.
3.
External oblique → external spermatic fascia.
4.
Processus vaginalis (peritoneum) → tunica vaginalis.
(ii)
Inguinal canal in children:
1.
Shorter in infants than adults as the external and internal ring are nearly effaced, which leads to increased risk of incarceration.
2.
Scarpa’s fascia well developed in children and may be mistaken for external oblique aponeurosis.
(c)
Embryology:
(i)
Gonads form at 5th week gestation within the retroperitoneal nephrogenic ridges.
(ii)
Testis descends to internal ring at seven months gestation.
(iii)
Testis descent mediated by calcitonin gene-related peptide (CGRP) released from the genitofemoral nerve.
(iv)
Descent of testis proceeds along gubernaculum and “drags” a diverticulum of peritoneum known as the processus vaginalis.
(v)
Obliteration of processus vaginalis mediated by CGRP.
(vi)
Failure of this obliteration leads to the potential for indirect inguinal hernia formation.
(vii)
Ovarian descent arrests within the pelvis.
(viii)
Left testicular descent precedes right side therefore right sided hernias are more common as the likelihood of PPV closure decreases after birth.
(d)
Incidence:
(i)
Undescended testis and PPV are more common in prematurity.
(ii)
Approximately 1 in 20 males will develop an inguinal hernia.
(iii)
Family history is positive in approximately 10 %.
(iv)
Incidence of inguinal herniation increases with prematurity and is estimated within 10–30 %.
(e)
Get Clinical Tree app for offline access

Associated Conditions:
(i)
Prematurity.
(ii)
Cryptorchidism (90 % have PPV).
(iii)
Connective tissue disorder.
(iv)
Cystic fibrosis.
(v)
Ascites.
(vi)




Abdominal wall defect.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree