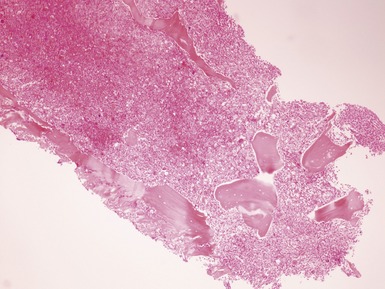
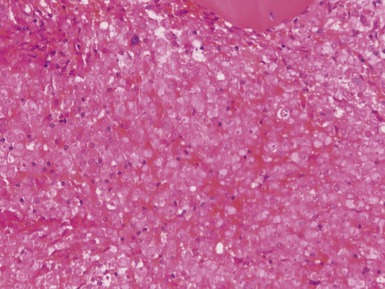
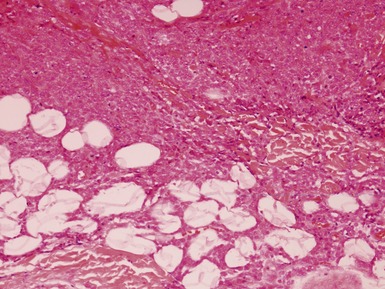
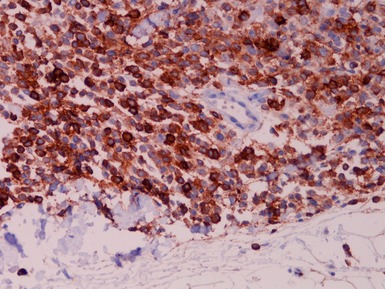
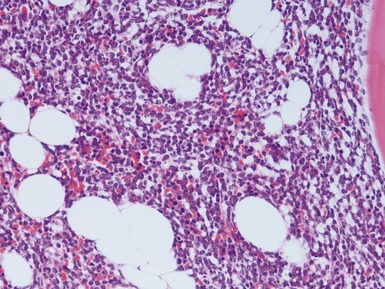
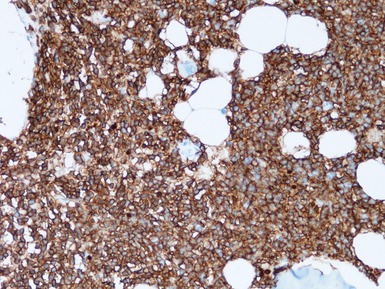
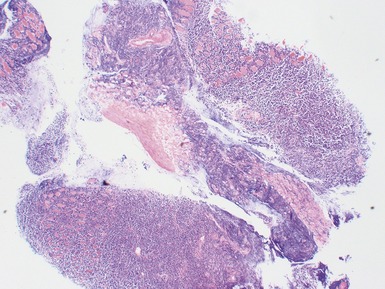
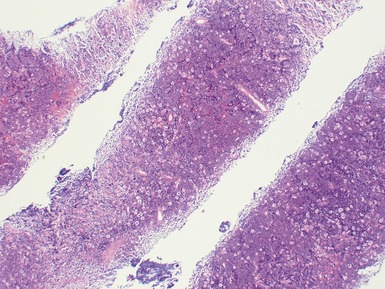
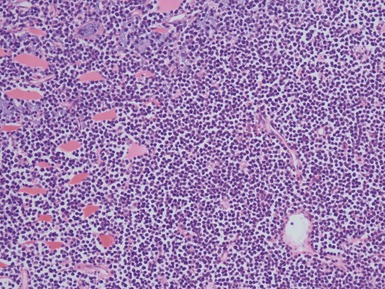
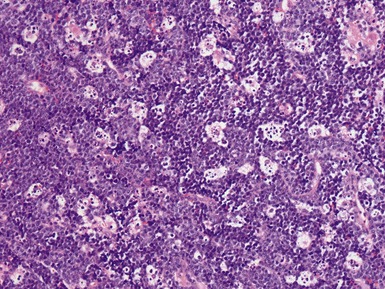
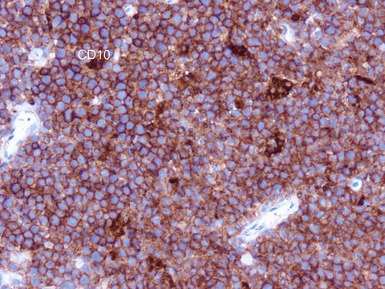
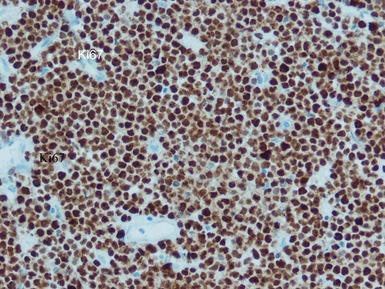
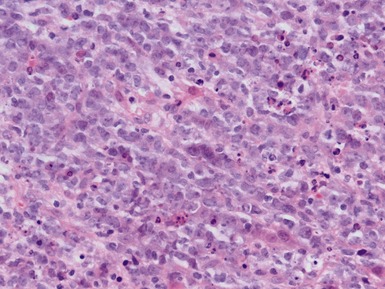
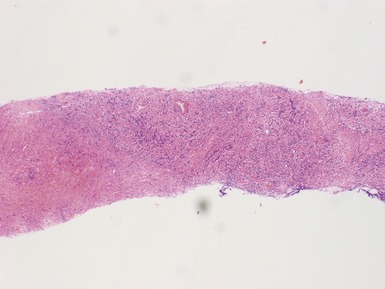
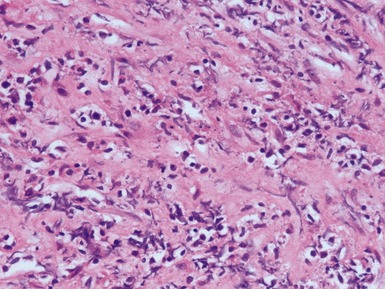
CHAPTER 8 HEMATOLYMPHOID PATHOLOGY Pediatric leukemia / lymphoma Introduction Acute myeloid leukemia (AML) Myeloid sarcoma Acute leukemia of ambiguous lineage Precursor b acute lymphoblastic leukemia / lymphoma Precursor t acute lymphoblastic leukemia / lymphoma Mature b cell leukemia / lymphoma Burkitt lymphoma Diffuse large b-cell lymphoma (DLBCL) Anaplastic large cell lymphoma (ALCL) Lymphomatoid granulomatosis Primary cutaneous cd30-positive t-cell lymphoproliferative disorders Peripheral t-cell lymphoma (UNSPECIFIED) Juvenile myelomonocytic leukemia (JMML) Hodgkin lymphoma Primary immunodeficiency associated lymphoproliferative disorders (LPDs) Post-transplant lymphoproliferative disorders (PTLD) Reactive lymphadenopathies Non-specific reactive lymphoid hyperplasia Viral lymphadenopathies Other infective lymphadenopathies Kimura lymphadenopathy Sinus histiocytosis with massive lymphadenopathy (rosai–dorfman disease) Kikuchi–fujimoto lymphadenopathy Lupus lymphadenopathy Castleman disease (angiofollicular lymph node hyperplasia) Histopathology of immunodeficiencies Introduction Autoimmune lymphoproliferative syndrome (alps) Langerhans cell histiocytosis PEDIATRIC LEUKEMIA / LYMPHOMA INTRODUCTION • Diagnostic features are generally same as adults but different distribution of entities, mainly: acute myeloid leukemia acute lymphoblastic leukemia / lymphoma (ALL) Burkitt lymphoma diffuse large B cell lymphoma anaplastic large cell lymphoma Hodgkin lymphoma juvenile myelomonocytic leukemia ACUTE MYELOID LEUKEMIA (AML) • Clonal expansion of myeloid blasts • Classified according to categories and subtypes (WHO) AML with recurrent genetic abnormalities AML with multilineage dysplasia therapy related AML AML not otherwise categorized – minimally differentiated through to lineage differentiation subtypes Epidemiology • Most AML occurs in adults represents around one-third of pediatric leukemia Histopathological features (Figs 8.1, 8.2) • Diagnosis requires blood and marrow aspirate with or without trephine • Increased myeloblasts • Trephine shows: increased cellularity – usually! – see pitfalls fibrosis specific features – see subtypes Fig. 8.1 Figs 8.1–8.2 Photomicrographs of bone marrow trephine biopsies from a child with acute myeloid leukemia, demonstrating marked infiltration of the marrow by sheets of myeloblasts. Immunohistochemical staining • Glycophorin for erythroid • CD61 for megakaryocytes • CD34 for immature precursors useful in hypocellular AML • TdT for blasts usually ALL • MPO, CD15, CD117 for myeloid differentiation • Nuclear WT1+ in a proportion of AML caution in interpretation of such staining in soft tissue lesions • Flow cytometry from aspirate is usually better for immunophenotyping than immunostaining of tissue sections Differential diagnoses and pitfalls • A minority of AML may present with hypocellular marrow • AML may present as granulocytic sarcoma always consider this possibility in an unusual soft tissue lesion AML with recurrent genetic abnormalities • Better prognosis as a group • Histopathological samples rarely allow such specific diagnosis requires genetic testing t(8;21)(q22;q22)(AML1/ETO) • 5–10% of AML mainly childhood cases • May present as granulocytic sarcoma • Myeloid markers + • Coexpression of CD19 • CD34+ • Variable TdT+ • CD56 expression associated with adverse prognosis Inv(16)(p13q22) or t(16;16)(p13;q22)(CBFb;MYH11) • 10% of AML mainly childhood cases • May present as granulocytic sarcoma • Eosinophilic granulocytes in marrow • Myeloid markers + lysozyme • FISH / RT-PCR required for diagnosis t(15;17)(q22;q12)(PML/RARa) • Acute promyelocytic leukemia 5% of AML – mainly adults • May present with DIC • Hypercellular marrow • Promyelocytes with granular cytoplasm • CD33, CD13, MPO+ • CD15− • Nuclear PML+ • Responds to transretinoic acid AML with 11q23 (MLL) abnormalities • 5% of AML more common in children – especially AML in infants • DIC with soft tissue infiltration • Monocytic / myelomonocytic phenotype • No specific immunohistochemical features AML NOS • >20% myeloblasts • Without specific molecular genetic features AML minimally differentiated • FAB M0 • 5% of AML mainly adults • Marrow failure • Medium sized blasts • Hypercellular marrow poorly differentiated blasts • CD117+ • CD34+ one-third • Sometimes lymphoid markers may also be focally positive • MPO, CD15 usually negative AML without maturation • FAB M1 • Extensive blasts without morphological differentiation • Marrow failure • Hypercellular marrow • MPO, CD34, CD117, lysozyme+ AML with maturation • FAB M2 30–40% of AML • AML with maturation to neutrophils • Marrow failure • Hypercellular marrow • Blasts and granulocyte differentiation • MPO, lysozyme, CD15, CD117, CD34+ • Some are translocation associated Acute myelomonocytic leukemia • FAB M4 • 15–25% of AML mainly adults • AML with neutrophil and monocyte differentiation • >20% marrow blasts • >20% monocyte differentiation • Marrow failure • MPO, CD36, CD64, lysozyme + • Subpopulation of CD34+ cells Acute monoblastic / monocytic leukemia • FAB M5 • >80% monocytic differentiation • 5% of AML mainly adults • Marrow failure with or without extramedullary masses • Hypercellular marrow with large blasts • Monoblasts lysozyme+ variable CD68+ MPO− • Other blasts MPO, CD117, lysozyme+ Acute erythroid leukemia • FAB M6 • 5% of AML mainly adults • Acute leukemia with >50% erythroid precursors if >80% then classify as pure erythroid • >20% of non-erythroid cells are myeloblasts • Hypercellular marrow • Erythroblasts MPO− glycophorin+ • Other blasts MPO, CD117, lysozyme + Acute megakaryoblastic leukemia • AML M7 • <5% of AML adults and children • Association with preceding mediastinal germ cell tumors in males • Poorly differentiated blasts and megakaryoblasts in marrow with variable fibrosis • May be associated with t(1;22) in infants • MPO− • CD41+, CD61+, Factor VIII RA+ variant is AML / transient myeloproliferative disorder in Trisomy 21 – neonates with T21 – increased blasts Acute basophilic leukemia • Rare <1% AML • Marrow blasts are CD34+ • Granular cytoplasm Acute panmyelosis with myelofibrosis • Rare • Variable increased marrow reticulin fibrosis with blasts • Variable expression of myeloid markers MPO, CD117, CD13, CD33 • Overlap with other AML with marrow fibrosis especially megakaryoblastic MYELOID SARCOMA (Figs 8.3–8.5) • Extramedullary mass of immature myeloid cells • Always consider the possibility in ‘odd’ sarcoma biopsies in children • May demonstrate nuclear WT1+ (Al Adnani et al 2007) • MPO, lysozyme, CD117, CD13, CD33, CD43 variably + • May be associated with concurrent AML or be apparently isolated Fig. 8.3 Figs 8.3–8.4 Photomicrographs of a granulocytic sarcoma presenting as an apparently primary soft tissue mass, demonstrating sheets of myeloblasts. Fig 8.5 Photomicrograph of a granulocytic sarcoma presenting as an apparently primary soft tissue mass, demonstrating sheets of myeloblasts, expressing myeloid markers, in this case lysozyme. ACUTE LEUKEMIA OF AMBIGUOUS LINEAGE • Some leukemias show neither diagnostic lymphoid nor myeloid features or mixtures of both • <5% acute leukemia • May express CD34 and/or TdT but no other specific diagnostic markers, or multiple markers of more than one lineage PRECURSOR B ACUTE LYMPHOBLASTIC LEUKEMIA / LYMPHOMA (Figs 8.6, 8.7) • Small to medium uniform B-lymphoblasts • Arbitrary definition of extramedullary sites with <25% blasts in marrow classified as lymphoma • 75% of ALL affects patients <6 years of age of these >80% are pre-B ALL • Diffuse uniform infiltration of marrow or extramedullary sites focal ‘starry sky pattern’ may also be seen • Nuclear TdT+ most useful marker, especially in extramedullary sites • CD19, CD79a+ • CD10 and CD20+ in most note that hematogones in marrow are also TdT and CD10+ • Ki67 index high but lower than Burkitt lymphoma usually 50–90% • Cytogenetic abnormalities in some cases may be related to prognosis • >70% overall survival Fig. 8.6 Figs 8.6–8.7 Photomicrographs of a case of acute pre B / common lymphoblastic leukemia, demonstrating extensive marrow involvement by sheets of bland, uniform lymphoblasts, which express nuclear TdT and membranous CD10 (shown in Fig 8.7) on immunostaining. PRECURSOR T ACUTE LYMPHOBLASTIC LEUKEMIA / LYMPHOMA • Small to medium sized uniform T-lymphoblasts • Arbitrary definition of extramedullary sites with <25% blasts in marrow classified as lymphoma • 15% of childhood ALL more common in adolescent males • Often with mediastinal or other tissue mass • Diffuse uniform infiltration of marrow or extramedullary sites • Focal ‘starry sky pattern’ may also be seen • Nuclear TdT+ • CD3/5+ • CD10, CD79a, CD13, CD33 may also be positive MATURE B CELL LEUKEMIA / LYMPHOMA • Clonal proliferations of B-cells in varying stages of maturity • May be associated with immunodeficiency or autoimmune disease in childhood • Some types are infection related EBV – Burkitt lymphoma HHV8 – primary effusion lymphoma H. pylori – mucosa associated lymphoid tissue • Many types are reported but in childhood almost all are: Burkitt lymphoma Diffuse large B-cell lymphoma (DLBCL) BURKITT LYMPHOMA Epidemiology • Endemic type Africa children 4–7 years almost all are EBV-related • Sporadic type all countries mainly children – <50% of childhood lymphoma <30% are EBV+ • Immunodeficiency-associated cases EBV+ in around 40% Genetics • Clonal immunoglobulin gene rearrangements • Classical translocation is t(8;14) results in MYC deregulation Clinical features • Often affects extranodal sites especially: – bone – jaw – ileum / cecum – ovaries – kidney – breast • Sporadic cases mainly present as abdominal masses • Risk of tumor lysis syndrome on treatment Histopathological features (Figs 8.8–8.14) • Monomorphic B-cell infiltration sheets of B-lymphocytes – round / ovoid nuclei – clumped chromatin – basophilic cytoplasm with lipid vacuoles numerous macrophages – starry sky pattern high proliferation rate – >95% with Ki67 staining • Variants: plasmacytoid atypical / Burkitt-like – increased pleomorphism Fig. 8.8 Fig. 8.9 Fig. 8.10 Figs 8.8–8.11 Photomicrographs of cases of Burkitt lymphoma, demonstrating sheets of uniform small ovoid B-lymphocytes, infiltrating surrounding tissue, with areas showing prominent tingible body macrophages (’starry sky pattern’). Fig. 8.12 Fig. 8.13 Figs 8.12–8.14 Photomicrographs of a case of Burkitt lymphoma, demonstrating immunoexpression of CD20, CD10 and almost 100% proliferation rate with Ki67 staining. Immunohistochemical staining • CD20 / CD79a+ • Usually CD10 + and bcl6+ • Ki67 >95% • TdT− DIFFUSE LARGE B-CELL LYMPHOMA (DLBCL) (Figs 8.15–8.18) • Large neoplastic B-cells more than twice normal size • Nodal or extranodal involvement • In childhood cases consider an underlying immunodeficiency • Diffuse infiltration by large B-cells often with centroblastic or immunoblastic differentiation • Variants: T-cell rich anaplastic plasmacytic ALK+ (CD30−) variants • CD19, CD20, CD79a+ • Variable Bcl2 and bcl6+ • Ki67 30–90% Fig. 8.15 Fig. 8.16 Figs 8.15–8.17 Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: METABOLIC DISEASE PATHOLOGY BONE PATHOLOGY RENAL PATHOLOGY TUMORS AND TUMOR-LIKE LESIONS Stay updated, free articles. Join our Telegram channel Join Tags: Diagnostic Pediatric Surgical Pathology Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on HEMATOLYMPHOID PATHOLOGY Full access? Get Clinical Tree
CHAPTER 8 HEMATOLYMPHOID PATHOLOGY Pediatric leukemia / lymphoma Introduction Acute myeloid leukemia (AML) Myeloid sarcoma Acute leukemia of ambiguous lineage Precursor b acute lymphoblastic leukemia / lymphoma Precursor t acute lymphoblastic leukemia / lymphoma Mature b cell leukemia / lymphoma Burkitt lymphoma Diffuse large b-cell lymphoma (DLBCL) Anaplastic large cell lymphoma (ALCL) Lymphomatoid granulomatosis Primary cutaneous cd30-positive t-cell lymphoproliferative disorders Peripheral t-cell lymphoma (UNSPECIFIED) Juvenile myelomonocytic leukemia (JMML) Hodgkin lymphoma Primary immunodeficiency associated lymphoproliferative disorders (LPDs) Post-transplant lymphoproliferative disorders (PTLD) Reactive lymphadenopathies Non-specific reactive lymphoid hyperplasia Viral lymphadenopathies Other infective lymphadenopathies Kimura lymphadenopathy Sinus histiocytosis with massive lymphadenopathy (rosai–dorfman disease) Kikuchi–fujimoto lymphadenopathy Lupus lymphadenopathy Castleman disease (angiofollicular lymph node hyperplasia) Histopathology of immunodeficiencies Introduction Autoimmune lymphoproliferative syndrome (alps) Langerhans cell histiocytosis PEDIATRIC LEUKEMIA / LYMPHOMA INTRODUCTION • Diagnostic features are generally same as adults but different distribution of entities, mainly: acute myeloid leukemia acute lymphoblastic leukemia / lymphoma (ALL) Burkitt lymphoma diffuse large B cell lymphoma anaplastic large cell lymphoma Hodgkin lymphoma juvenile myelomonocytic leukemia ACUTE MYELOID LEUKEMIA (AML) • Clonal expansion of myeloid blasts • Classified according to categories and subtypes (WHO) AML with recurrent genetic abnormalities AML with multilineage dysplasia therapy related AML AML not otherwise categorized – minimally differentiated through to lineage differentiation subtypes Epidemiology • Most AML occurs in adults represents around one-third of pediatric leukemia Histopathological features (Figs 8.1, 8.2) • Diagnosis requires blood and marrow aspirate with or without trephine • Increased myeloblasts • Trephine shows: increased cellularity – usually! – see pitfalls fibrosis specific features – see subtypes Fig. 8.1 Figs 8.1–8.2 Photomicrographs of bone marrow trephine biopsies from a child with acute myeloid leukemia, demonstrating marked infiltration of the marrow by sheets of myeloblasts. Immunohistochemical staining • Glycophorin for erythroid • CD61 for megakaryocytes • CD34 for immature precursors useful in hypocellular AML • TdT for blasts usually ALL • MPO, CD15, CD117 for myeloid differentiation • Nuclear WT1+ in a proportion of AML caution in interpretation of such staining in soft tissue lesions • Flow cytometry from aspirate is usually better for immunophenotyping than immunostaining of tissue sections Differential diagnoses and pitfalls • A minority of AML may present with hypocellular marrow • AML may present as granulocytic sarcoma always consider this possibility in an unusual soft tissue lesion AML with recurrent genetic abnormalities • Better prognosis as a group • Histopathological samples rarely allow such specific diagnosis requires genetic testing t(8;21)(q22;q22)(AML1/ETO) • 5–10% of AML mainly childhood cases • May present as granulocytic sarcoma • Myeloid markers + • Coexpression of CD19 • CD34+ • Variable TdT+ • CD56 expression associated with adverse prognosis Inv(16)(p13q22) or t(16;16)(p13;q22)(CBFb;MYH11) • 10% of AML mainly childhood cases • May present as granulocytic sarcoma • Eosinophilic granulocytes in marrow • Myeloid markers + lysozyme • FISH / RT-PCR required for diagnosis t(15;17)(q22;q12)(PML/RARa) • Acute promyelocytic leukemia 5% of AML – mainly adults • May present with DIC • Hypercellular marrow • Promyelocytes with granular cytoplasm • CD33, CD13, MPO+ • CD15− • Nuclear PML+ • Responds to transretinoic acid AML with 11q23 (MLL) abnormalities • 5% of AML more common in children – especially AML in infants • DIC with soft tissue infiltration • Monocytic / myelomonocytic phenotype • No specific immunohistochemical features AML NOS • >20% myeloblasts • Without specific molecular genetic features AML minimally differentiated • FAB M0 • 5% of AML mainly adults • Marrow failure • Medium sized blasts • Hypercellular marrow poorly differentiated blasts • CD117+ • CD34+ one-third • Sometimes lymphoid markers may also be focally positive • MPO, CD15 usually negative AML without maturation • FAB M1 • Extensive blasts without morphological differentiation • Marrow failure • Hypercellular marrow • MPO, CD34, CD117, lysozyme+ AML with maturation • FAB M2 30–40% of AML • AML with maturation to neutrophils • Marrow failure • Hypercellular marrow • Blasts and granulocyte differentiation • MPO, lysozyme, CD15, CD117, CD34+ • Some are translocation associated Acute myelomonocytic leukemia • FAB M4 • 15–25% of AML mainly adults • AML with neutrophil and monocyte differentiation • >20% marrow blasts • >20% monocyte differentiation • Marrow failure • MPO, CD36, CD64, lysozyme + • Subpopulation of CD34+ cells Acute monoblastic / monocytic leukemia • FAB M5 • >80% monocytic differentiation • 5% of AML mainly adults • Marrow failure with or without extramedullary masses • Hypercellular marrow with large blasts • Monoblasts lysozyme+ variable CD68+ MPO− • Other blasts MPO, CD117, lysozyme+ Acute erythroid leukemia • FAB M6 • 5% of AML mainly adults • Acute leukemia with >50% erythroid precursors if >80% then classify as pure erythroid • >20% of non-erythroid cells are myeloblasts • Hypercellular marrow • Erythroblasts MPO− glycophorin+ • Other blasts MPO, CD117, lysozyme + Acute megakaryoblastic leukemia • AML M7 • <5% of AML adults and children • Association with preceding mediastinal germ cell tumors in males • Poorly differentiated blasts and megakaryoblasts in marrow with variable fibrosis • May be associated with t(1;22) in infants • MPO− • CD41+, CD61+, Factor VIII RA+ variant is AML / transient myeloproliferative disorder in Trisomy 21 – neonates with T21 – increased blasts Acute basophilic leukemia • Rare <1% AML • Marrow blasts are CD34+ • Granular cytoplasm Acute panmyelosis with myelofibrosis • Rare • Variable increased marrow reticulin fibrosis with blasts • Variable expression of myeloid markers MPO, CD117, CD13, CD33 • Overlap with other AML with marrow fibrosis especially megakaryoblastic MYELOID SARCOMA (Figs 8.3–8.5) • Extramedullary mass of immature myeloid cells • Always consider the possibility in ‘odd’ sarcoma biopsies in children • May demonstrate nuclear WT1+ (Al Adnani et al 2007) • MPO, lysozyme, CD117, CD13, CD33, CD43 variably + • May be associated with concurrent AML or be apparently isolated Fig. 8.3 Figs 8.3–8.4 Photomicrographs of a granulocytic sarcoma presenting as an apparently primary soft tissue mass, demonstrating sheets of myeloblasts. Fig 8.5 Photomicrograph of a granulocytic sarcoma presenting as an apparently primary soft tissue mass, demonstrating sheets of myeloblasts, expressing myeloid markers, in this case lysozyme. ACUTE LEUKEMIA OF AMBIGUOUS LINEAGE • Some leukemias show neither diagnostic lymphoid nor myeloid features or mixtures of both • <5% acute leukemia • May express CD34 and/or TdT but no other specific diagnostic markers, or multiple markers of more than one lineage PRECURSOR B ACUTE LYMPHOBLASTIC LEUKEMIA / LYMPHOMA (Figs 8.6, 8.7) • Small to medium uniform B-lymphoblasts • Arbitrary definition of extramedullary sites with <25% blasts in marrow classified as lymphoma • 75% of ALL affects patients <6 years of age of these >80% are pre-B ALL • Diffuse uniform infiltration of marrow or extramedullary sites focal ‘starry sky pattern’ may also be seen • Nuclear TdT+ most useful marker, especially in extramedullary sites • CD19, CD79a+ • CD10 and CD20+ in most note that hematogones in marrow are also TdT and CD10+ • Ki67 index high but lower than Burkitt lymphoma usually 50–90% • Cytogenetic abnormalities in some cases may be related to prognosis • >70% overall survival Fig. 8.6 Figs 8.6–8.7 Photomicrographs of a case of acute pre B / common lymphoblastic leukemia, demonstrating extensive marrow involvement by sheets of bland, uniform lymphoblasts, which express nuclear TdT and membranous CD10 (shown in Fig 8.7) on immunostaining. PRECURSOR T ACUTE LYMPHOBLASTIC LEUKEMIA / LYMPHOMA • Small to medium sized uniform T-lymphoblasts • Arbitrary definition of extramedullary sites with <25% blasts in marrow classified as lymphoma • 15% of childhood ALL more common in adolescent males • Often with mediastinal or other tissue mass • Diffuse uniform infiltration of marrow or extramedullary sites • Focal ‘starry sky pattern’ may also be seen • Nuclear TdT+ • CD3/5+ • CD10, CD79a, CD13, CD33 may also be positive MATURE B CELL LEUKEMIA / LYMPHOMA • Clonal proliferations of B-cells in varying stages of maturity • May be associated with immunodeficiency or autoimmune disease in childhood • Some types are infection related EBV – Burkitt lymphoma HHV8 – primary effusion lymphoma H. pylori – mucosa associated lymphoid tissue • Many types are reported but in childhood almost all are: Burkitt lymphoma Diffuse large B-cell lymphoma (DLBCL) BURKITT LYMPHOMA Epidemiology • Endemic type Africa children 4–7 years almost all are EBV-related • Sporadic type all countries mainly children – <50% of childhood lymphoma <30% are EBV+ • Immunodeficiency-associated cases EBV+ in around 40% Genetics • Clonal immunoglobulin gene rearrangements • Classical translocation is t(8;14) results in MYC deregulation Clinical features • Often affects extranodal sites especially: – bone – jaw – ileum / cecum – ovaries – kidney – breast • Sporadic cases mainly present as abdominal masses • Risk of tumor lysis syndrome on treatment Histopathological features (Figs 8.8–8.14) • Monomorphic B-cell infiltration sheets of B-lymphocytes – round / ovoid nuclei – clumped chromatin – basophilic cytoplasm with lipid vacuoles numerous macrophages – starry sky pattern high proliferation rate – >95% with Ki67 staining • Variants: plasmacytoid atypical / Burkitt-like – increased pleomorphism Fig. 8.8 Fig. 8.9 Fig. 8.10 Figs 8.8–8.11 Photomicrographs of cases of Burkitt lymphoma, demonstrating sheets of uniform small ovoid B-lymphocytes, infiltrating surrounding tissue, with areas showing prominent tingible body macrophages (’starry sky pattern’). Fig. 8.12 Fig. 8.13 Figs 8.12–8.14 Photomicrographs of a case of Burkitt lymphoma, demonstrating immunoexpression of CD20, CD10 and almost 100% proliferation rate with Ki67 staining. Immunohistochemical staining • CD20 / CD79a+ • Usually CD10 + and bcl6+ • Ki67 >95% • TdT− DIFFUSE LARGE B-CELL LYMPHOMA (DLBCL) (Figs 8.15–8.18) • Large neoplastic B-cells more than twice normal size • Nodal or extranodal involvement • In childhood cases consider an underlying immunodeficiency • Diffuse infiltration by large B-cells often with centroblastic or immunoblastic differentiation • Variants: T-cell rich anaplastic plasmacytic ALK+ (CD30−) variants • CD19, CD20, CD79a+ • Variable Bcl2 and bcl6+ • Ki67 30–90% Fig. 8.15 Fig. 8.16 Figs 8.15–8.17 Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: METABOLIC DISEASE PATHOLOGY BONE PATHOLOGY RENAL PATHOLOGY TUMORS AND TUMOR-LIKE LESIONS Stay updated, free articles. Join our Telegram channel Join Tags: Diagnostic Pediatric Surgical Pathology Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on HEMATOLYMPHOID PATHOLOGY Full access? Get Clinical Tree