1 Health Status of Children
Global and Local Perspectives
More than 20 years ago, the United Nations (UN) Children’s Fund (UNICEF) held the Convention on the Rights of Children and enacted a legal document asserting a broad range of human rights inherently due to children. Children, because of their vulnerability, need special care and protection (Forum on Child and Family Statistics, 2010; UNICEF, 2009). The United Nations Convention on the Rights of Children (UNCRC) sets minimum entitlements and freedoms that should be respected by governments. Box 1-1 presents a summary of the articles from the Convention that addresses the rights of protection (UNICEF, 2009). The document applies to children globally and is founded on respect for the dignity and worth of each individual, regardless of race, color, gender, language, religion, opinions, origins, wealth, birth status, or ability. Unfortunately there are many children who do not live in nurturing family environments and who lack freedom from armed conflict, violence, and exploitation. The UNCRC continues to work on ensuring that all children have basic human rights and freedoms.
BOX 1-1 Convention on the Rights of the Child: Summary of Protection Rights
From United Nations International Children’s Fund: The state of the world’s children, ed 2, New York, 2009, UNICEF, p 25.
| Articles | |
|---|---|
| Illicit transfers and illegal adoption | 11, 21 |
| Violence, abuse, exploitation, and neglect | 19 |
| Armed conflict | 22, 38-39 |
| Child labor, trafficking, sexual and other forms of exploitation, and drug abuse | 32-36, 39 |
| Torture and deprivation of liberty, and capital punishment | 37-39 |
In addition, the Convention ensures special protection, assistance and care for children who are:
| Deprived of the family environment | 20, 22 |
| Disabled | 23 |
| In conflict with the law | 37, 39-40 |
 Global Health Status of Children
Global Health Status of Children
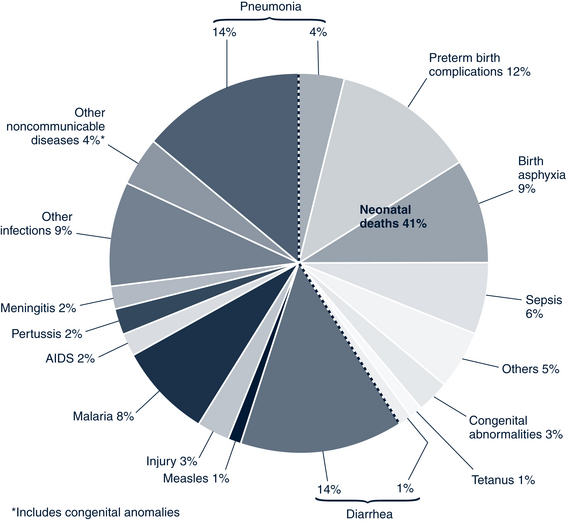
Successful vaccination programs have markedly reduced the mortality caused by some infectious diseases, particularly measles and tetanus; however, tetanus is still responsible for 1% of deaths in children younger than 5 years of age. Figure 1-1 illustrates the global, regional, and national causes of child mortality (Black et al, 2010).
Millennium Development Goals
The UN Millennium Development Goals aim to reduce childhood mortality by two thirds in children younger than 5 years of age by 2015 and to provide benchmarks for tackling extreme poverty both globally and locally (United Nations, 2000). The eight goals consist of 21 quantifiable targets that are measured by 60 health indicators (Fig. 1-2). They provide a framework for the international community to ensure socioeconomic development reaches all children. If these goals are achieved, poverty could be reduced by 50% worldwide. To reach this goal, expansion and acceleration of the interventions by the WHO to target the leading causes of death are required in the target countries.

Food Insecurity and Effect on Child Health
Hunger and undernutrition are often referred to as food insecurity, the condition that exists when people do not have “physical and economic access to sufficient, safe, nutritious, and culturally acceptable food to meet their dietary needs” (United Nations Millennium Project, 2006, p 20). Poverty and food insecurity are primary contributors to maternal and child undernutrition. Food insecurity occurs in impoverished populations in developing countries and in industrialized nations particularly among migrant populations. Children affected by migration and family separation are at risk for food insecurity and are vulnerable to further health consequences including exposure to exploitation and child trafficking. Growing evidence on climate change indicates the dramatic effect on food crops that lead to food distribution issues, one of the primary contributors to food insecurity. Figure 1-3 illustrates the relationship between climate change, food availability, and malnutrition.
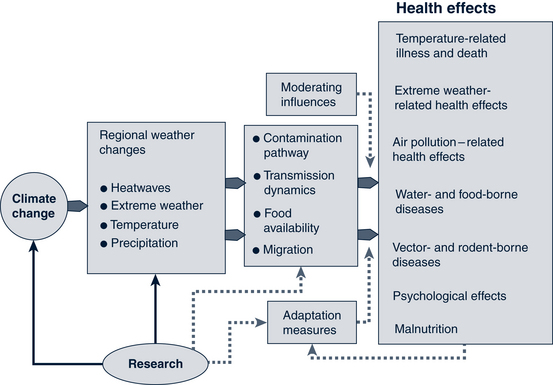
FIGURE 1-3 Pathways by which climate change affects health.
(Used with permission from World Health Organization: Children’s health & environment: a review of the evidence, p 29, 2002. [WHO adapted from Patz JA, McGeehin MA, Bernard SM et al: The potential health impacts of climate variability and change for the United States: executive summary of the report of the health sector of the US National Assessment, Environ Health Perspectives,108:367-376, 2000]).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


