Figure 5.1 DNA – the Nobel Prize winning description of the double helix.
Source: Watson and Crick (1953).

The base pair structure of DNA allows replication. During cell division, chromosomes align, replicate and divide. In mitosis, identical diploid daughter cells result. In meiosis, haploid gametes are produced: eggs and sperm containing half the genetic material, with just one of each of the pairs of chromosomes. In meiosis, genetic material may be swapped between chromosomes, while all cell division carries potential for mutation.
Genes code for polypeptide sequences and these may constitute or may be built into proteins. Post-translational changes modify structure and function and result in functional proteins.
The potential for errors is massive, but most do not result in disease. It is important to understand the principles underlying genetic disease for diagnosis, prognosis, treatment and genetic counselling.
For any characteristic (height, blood pressure, etc.), our phenotype (the way we are) is the result of complex interaction between our genotype (genetic material related to that characteristic) and our environment (Figure 5.2).
 RESOURCE
RESOURCE5.2 Genetic mechanisms of disease
- Chromosomal
- Abnormal number (aneuploidy)
- Translocation (balanced or unbalanced)
- Duplication
- Deletion
- Copy number variation (abnormal numbers of copies of section of DNA)
- Abnormal number (aneuploidy)
- Single gene disorders
- Mutations
- Missense (protein product is abnormal, e.g. amino acid substitution)
- Nonsense (protein product is not complete)
- Missense (protein product is abnormal, e.g. amino acid substitution)
- Mutations
- Triplet repeat (base pair triplets)
- Gene imprinting (e.g. modification of gene expression by gender of parent)
- Mitochondrial DNA abnormalities
- Multifactorial inheritance
5.2.1 Chromosomal abnormalities
Aneuploidy means that there is an extra chromosome (e.g. Trisomy 21, Down syndrome; 47XXY, Klinefelter syndrome) or one missing (e.g. 45XO, Turner syndrome). Most aneuploidy arises because of non-disjunction (failure of the pair of chromosomes to separate), and often it results in spontaneous miscarriage. Down syndrome (trisomy 21), Edward syndrome (trisomy 18), Patau syndrome (trisomy 13) and the sex chromosome aneuploidies account for most infants with abnormal chromosome number. Risk of Down syndrome aneuploidy rises with maternal age.
Figure 5.3 A balanced 21 translocation in a healthy parent can result in Down syndrome in the child.
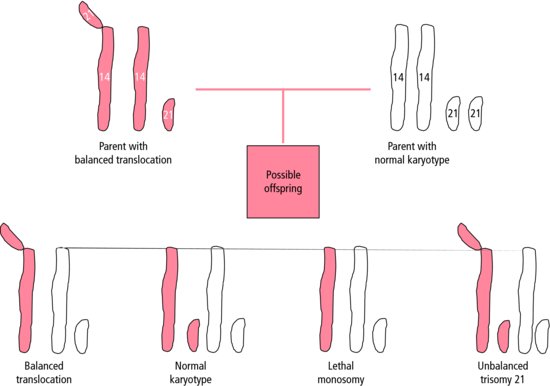
Translocations occur when a part of one chromosome is stuck to another. If the total chromosome content is normal or near normal (a balanced translocation), the phenotype may be normal. The risk for this person is that their offspring may inherit an unbalanced karyotype.
The other chromosomal abnormalities are associated with a wide variety of phenotypes. Some deletions or duplications may be a chance finding in a healthy child or their family. On the other hand, some are small and not visible on microscopy, yet may result in a variety of important syndromic abnormalities (e.g. 22q deletions: Di George syndrome spectrum with hypocalcaemia, T-cell deficiency, cardiac defects).
 A syndrome is a phenotype with a recognizable pattern of various abnormalities or problems.
A syndrome is a phenotype with a recognizable pattern of various abnormalities or problems.5.2.2 Single gene disorders
These may adopt the classical Mendelian patterns of inheritance.
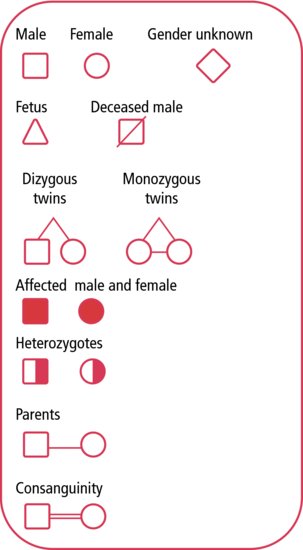
Symbols for a genetic pedigree are shown in Figure 5.4.
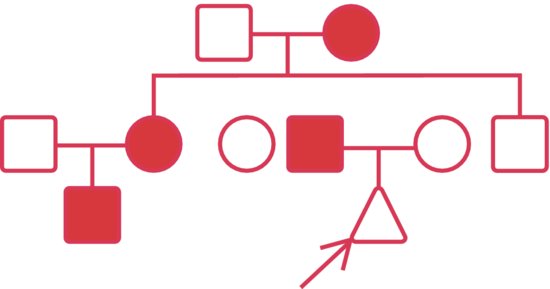
5.2.2.1 Autosomal dominant (Figure 5.5)
- Parents affected
- Females and males affected
- Female and male transmission
- 50% recurrence risk
- High new mutation rates
- Variable penetrance in some conditions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


