Chapter 62 Genetics
What Are the Reasons for a Genetic Consultation?

 Growth problems, including short stature, failure to thrive, or overgrowth
Growth problems, including short stature, failure to thrive, or overgrowth

 Premature or delayed puberty or ambiguous genitalia
Premature or delayed puberty or ambiguous genitalia
 Prenatal exposure to alcohol, drugs, or other teratogens
Prenatal exposure to alcohol, drugs, or other teratogens
 Recurrent miscarriages or advanced maternal age
Recurrent miscarriages or advanced maternal age
 Family history of a known disorder, such as cystic fibrosis or fragile X syndrome
Family history of a known disorder, such as cystic fibrosis or fragile X syndrome

BIRTH DEFECTS
ETIOLOGY
What Causes Birth Defects?
 Single-gene disordersmay have autosomal dominant, autosomal recessive, X-linked recessive, or X-linked dominant inheritance. There are now more than 5000 such disorders recognized. It is estimated that single-gene disorders affect 2% of the general population over a lifetime and 6% to 8% of hospitalized children.
Single-gene disordersmay have autosomal dominant, autosomal recessive, X-linked recessive, or X-linked dominant inheritance. There are now more than 5000 such disorders recognized. It is estimated that single-gene disorders affect 2% of the general population over a lifetime and 6% to 8% of hospitalized children.



EVALUATION
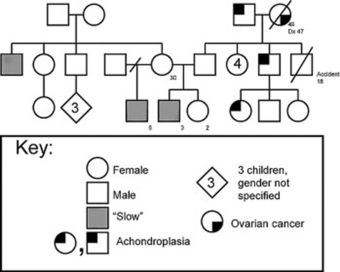
How Do I Develop a Family Pedigree?
A family pedigree is essential to help determine whether an identifiable mode of inheritance can explain the presenting problem: autosomal dominant, autosomal recessive, X-linked, or chromosome translocation. The family history is recorded in a pedigree with symbols representing individuals and their symptoms or disorders. At least three generationsare needed to establish inheritance patterns. If the pedigree shows male-to-male transmission, an equal number of males and females affected, and affected individuals in each successive generation, this confirms autosomal dominant inheritance.If males are predominantly affected on the maternal side of the family and vertical transmission is demonstrated, then X-linked inheritanceis likely. Horizontal patterns of affected individuals or siblings, or consanguinity (relatedness), suggest autosomal recessive inheritance.The family history is recorded in a pedigree with symbols representing individuals and their symptoms or disorders (Figure 62-1).
What Is Important on Physical Examination?
The physical examination must look for minor and major structural anomalies and specifically note the physical growth of various parts of the body such as upper and lower segment measurements or size of the ears. This requires careful measurements to provide quantitative assessment and comparison with established norms. There are published graphs of these measures (Hall et al., 1995).
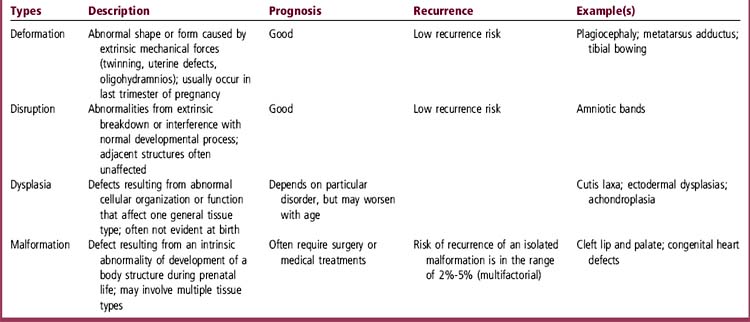
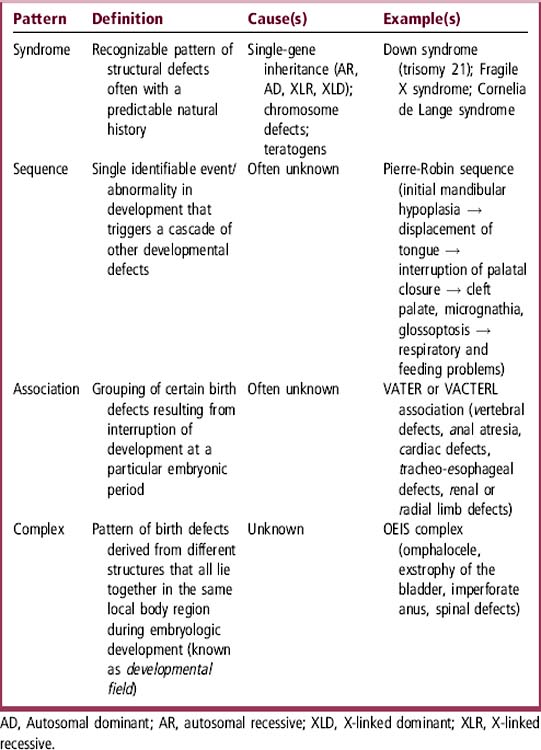
Do Multiple Birth Defects Have Recognizable Patterns?
Multiple major and minor structural anomalies can have recognizable patterns: syndrome, sequence, association, and complex. Table 62-2defines and gives examples of each pattern. Each of these patterns has implications for etiology, natural history, and prognosis. The patterns of malformationmust be considered when a child has multiple major and minor anomalies, especially if accompanied by growth, developmental, or behavioral abnormalities. Each pattern may have different modes of inheritance: single gene, chromosome abnormality, or multifactorial causes.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


