108 Gastritis and Gastrointestinal Bleeding
Etiology and Pathogenesis
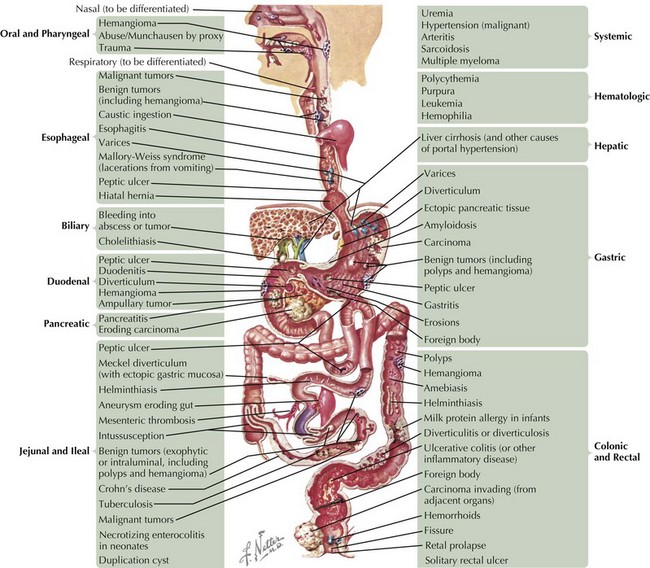
The causes of GI bleeding are diverse (Figure 108-1). Although the sheer number of causes may seem intimidating, grouping them into pathophysiologic categories aids in constructing a differential diagnosis. Note that underlying disorders of coagulation (e.g., hemophilias, vitamin K deficiency in neonates) and hepatic dysfunction (caused by the liver’s role in producing coagulation factors) can exacerbate any of these causes.
Mucosal Erosion
Inflammation
Disruption of mucosal integrity may occur in disorders that promote the recruitment of inflammatory cells, such as lymphocytes and neutrophils, which injure the epithelium by direct cell-to-cell contact or via secreted immunologic factors, such as cytokines. Examples include autoimmune enteropathy and eosinophilic gastroenteritis. Another important example is inflammatory bowel disease, a complex autoimmune disease that encompasses Crohn’s disease, which can cause full-thickness inflammation anywhere along the GI tract, and ulcerative colitis, which causes mucosal ulcerations in the colon (see Chapter 110). Children who have undergone bone marrow transplant may experience a form of rejection called graft-versus-host disease (GVHD). When it affects the GI tract, GVHD causes diarrhea, vomiting, fever, abdominal pain, and GI bleeding. Certain immunodeficiencies, such as common variable immunodeficiency, precipitate inflammation because of dysregulated immunity that leads to autoimmune responses (see Chapter 21).
Infection
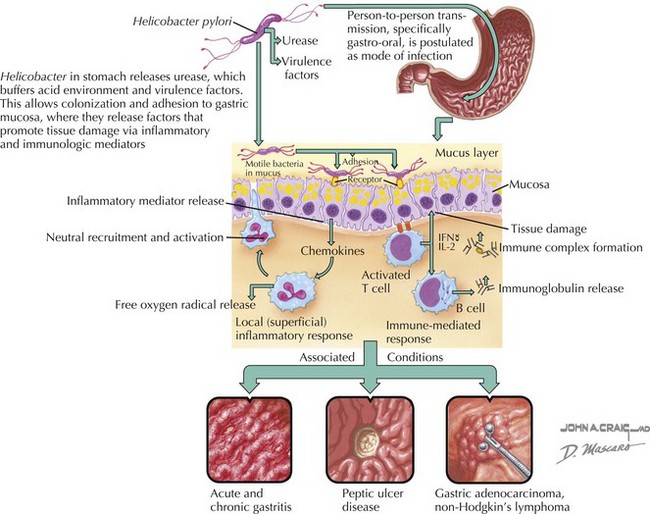
Infections disrupt mucosal integrity by direct cytotoxicity and/or by promoting inflammation. For example, herpes simplex virus is known to cause florid esophagitis, particularly in immunocompromised individuals, with nearly one-third of these patients experiencing an acute upper GI bleed. Additionally, infections may elicit specific peculiar responses. For example, cytomegalovirus is occasionally associated with massive gastric epithelial proliferation leading to a hypertrophic gastropathy called Menetrier’s disease. This causes protein wasting (including coagulation factors) from the leaky mucosa, as well as a higher risk of mucosal erosion and bleeding. Helicobacter pylori is perhaps the most infamous of the infectious causes of gastritis and duodenitis because of its chronicity, high prevalence (especially in certain populations of children, such as immigrants, the poor, and those attending daycare centers), its associations with peptic ulcers and adenocarcinoma of the stomach and duodenum, and its resistance to eradication (Figure 108-2).
Vascular Abnormalities
Congenital vascular defects may result in fragile vascular arrangements vulnerable to erosive and mechanical insults. Whereas hemangiomas represent proliferative vessel abnormalities that may regress, true malformations (including disorders such as arteriovenous malformations, blue rubber bleb nevus syndrome, and Osler-Rendu-Weber syndrome) are nonproliferative and do not regress. Processes that compromise the full thickness of bowel, such as Crohn’s disease and bowel surgery, may result in vessel-to-bowel fistulas associated with significant bleeding. Vasculitides, such as Henoch-Schönlein purpura, may result in occlusion of mesenteric vessels and intestinal ischemia (see Chapter 28).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


