Mixed echos, may include cystic areas, hemorrhage or calcification
calcifications
Right sided
May be very large
Central nervous system tumors
CNS tumors comprise 10% of all prenatally diagnosed tumors with most being supratentorial, in marked contrast to pediatric tumors, which are mostly infratentorial[2]. Generally the prognosis is poor and worse if the diagnosis is made prior to 30 weeks where mortality secondary to severe hydrocephalus can be up to 96%[3].
Most CNS tumors will be identified as an intracranial mass with associated hydrocephalus, macrocephaly or polyhydramnios. The mainstay of diagnosis should be to identify potentially curable CNS tumors, such as choroid plexus papillomas, from rapidly fatal ones, such as teratomas or neuroepithelial tumors. The use of fetal MRI may aid determination of tissue type.
Hydrocephalus and macrocephaly develop secondary to obstruction of the ventricular system and cerebrospinal fluid outflow. Rapid growth of a tumor may also lead to macrocephaly secondary to tumor size or the development of hydrops due to cardiovascular compromise. Twenty-one percent of fetuses with CNS tumors will be stillborn as a result of these complications[4]. Due to the high incidence of hemorrhage (18%) in CNS tumors, all diagnoses of intracranial hemorrhage should include assessment of the possibility of an underlying brain lesion. Pediatric neurosurgeons should be involved in the development of a multidisciplinary management plan. Delivery may be complicated by the presence of significant macrocephaly and cesarean section or predelivery decompression of the skull may be required to prevent labor dystocia.
Teratoma
Although rare in older children, intracranial teratoma is the most common CNS tumor in the fetus (>50%)[5]. Most will be located within the ventricles, hypothalamic, suprasellar or cerebral regions. As with all teratomas, they appear as an irregular solid and cystic echogenic mass with calcifications that distort the normal appearance of the brain. Teratomas comprise tissue from all three germ cell layers with immature neuroglial elements. Prognosis is extremely poor and is related to the size of the tumor and presence of associated hydrocephalus. A third will die in utero with only 12% surviving the neonatal period and 7% reaching 1 year of age[5].
Astrocytomas
Astrocytomas are the second most common congenital CNS tumor and represent a wide range of pathologies from subependymal giant cell astrocytomas to glioblastoma multiforme[5]. The appearances on ultrasound are of a unilateral echogenic mass within the cerebral hemisphere, which may have internal hemorrhage and often causes midline shift. The prognosis is generally poor with 13% stillborn and 37% surviving the neonatal period. The situation is even worse in the more aggressive glioblastoma multiforme where only 13% will survive[4].
Ependymoma
Ependymomas are tumors of the ependymal cells lining the ventricles or spinal canal. Ultrasound appearances are of mixed echogenic masses arising from the ventricle, which may include cystic areas, hemorrhage or calcification. They commonly arise from the fourth ventricle. There can be extension into the subarachnoid space with resultant involvement of the spinal cord. Macrocephaly and hydrocephalus are common features, and stillbirth, intracerebral hemorrhage and labor dystocia are complications.
Neuroepithelial tumors/medulloblastoma
Tumors comprised of neuroepithelial tissue can be termed primitive neuroepithelial tumors or medulloblastoma, and whilst common in the pediatric population, this is a much less common finding in the perinatal period. Unlike most other perinatal CNS tumors they are often infratentorial, arising from the cerebellar vermis and extending into the fourth ventricle. Survival is very poor at 12%[6].
Choroid plexus tumor
Tumors of the choroid plexus are rare and mostly papillomas or occasionally carcinomas. They represent 20% of congenital brain tumors and are less common in older children. The hallmark of choroid plexus tumors is excessive cerebrospinal fluid (CSF) production with associated hydrocephalus and macrocephaly. The appearance on ultrasound is of a large lobulated highly echogenic (cauliflower-like) mass, usually unilateral and located in the atria of the lateral ventricle, or rarely in the third ventricle. Treatment is with surgical excision, with adjuvant chemotherapy and radiotherapy for carcinoma, and survival rates of >70% are common[5].
Craniopharyngioma
These tumors are rare in the perinatal period. When found, they present as large heterogeneous cystic lesions with calcifications. They arise in the suprasellar region from epithelial origin. The prognosis is worse when identified in the perinatal period.
Spinal cord tumors
Congenital tumors of the spinal cord are extremely rare and most commonly are actually saccrococcygeal teratomas. Occasionally astrocytomas can present in this location, and as with most CNS tumors the prognosis is poor.
Differential diagnoses: CNS cysts and vascular malformations
Whilst technically not tumors, these lesions are included as they are important differential diagnoses when investigating CNS lesions.
Choroid plexus cysts
These fluid-filled cystic areas are located within the choroid plexus and form during normal development. They can be found in up to 1% of fetuses on routine ultrasound scanning where they appear as well-circumscribed sonolucent, unilocular or septated cysts >3 mm diameter within the choroid plexus itself. They tend to resolve by the third trimester or soon after birth. They have historically been linked to chromosomal disorders such as trisomy 18, but this risk is low and if found in isolation, does not warrant invasive testing.
Particularly large cysts are usually unilateral and may lead to ventriculomegaly due to obstruction of the flow of cerebrospinal fluid, but in invariably the outcomes are good[7]. Treatment in the neonatal period may be required with removal or fenestration techniques.
Arachnoid cysts
These cysts are benign congenital collections of CSF and may account for 1% of all CNS masses in children. The cysts are lined with collagen arising from the arachnoid mater and there may be communication to the subarachnoid space. Ultrasound appearances are of peripherally placed discrete sonolucent lesion with thin, smooth walls. They are usually supratentorial with the majority located within the sylvian fissure, but they may be found in the posterior fossa[8].
The main effect of arachnoid cysts is as a space-occupying lesion, and therefore the size and location of the cysts can be critical to prognosis. Small cysts may be of no clinical importance, whereas large cysts may cause seizures and neurologic symptoms in the newborn period. Isolated cysts usually have a good prognosis, although regular follow-up is required as they may increase in size in the third trimester leading to the development of hydrocephaly, particularly if located in the posterior fossa. Intrauterine cyst drainage has been attempted for the rapidly enlarging cyst, but usually this can be deferred until after birth.
Arachnoid cysts are usually isolated lesions, but they may be associated with other CNS malformations, such as agenesis of the corpus callosum, absent septum pellucidum, Arnold–Chiari malformation type I, and a variety of chromosomal/genetic syndromes, such as distichiasis-lymphedema, Mohr syndrome, trisomy 18, triploidy and unbalanced translocations. Therefore, amniocentesis should be offered in all cases of arachnoid cysts due to the association with genetic anomalies.
Vein of Galen aneurysm
Aneurysm of the great cerebral vein (of Galen) is extremely rare but relatively easy to diagnose with approximately 50% being diagnosed before infancy. The vein of Galen is part of the network of deep cerebral veins and curves under the splenium of the corpus callosum joining with the inferior sagittal sinus to form the straight sinus. This aneurysmal defect occurs as a result of an arteriovenous malformation between the primitive choroidal vessels and the median prosencephalic vein of Markowski.
Ultrasound appearances are of a well-defined midline sonolucent mass above the corpus callosum and cerebellum extending to the cranium. The use of color Doppler shows a nonpulsatile turbulent flow within the dilated vessel. Additional features within the head include macrocephaly or hydrocephalus. Fetal MRI is important to detect other anomalies and to exclude other differential diagnoses, such as arachnoid, porencephalic or choroid plexus cysts. Common complications include hydrocephaly, high-output cardiac failure and stillbirth. Other sequelae of a vein of Galen aneurysm may occur within the rest of the fetus, and include cardiomegaly, pericardial effusion, dilated neck veins, hepatomegaly, ascites, polyhydramnios and hydrops fetalis. In addition, ballantyne (mirror) syndrome may also present due to a hydropic placenta.
The prognosis for antenatally diagnosed vein of Galen aneurysms is related to the presence of associated cardiac or cerebral anomalies. When other anomalies are present the outcome is invariably poor[9]. For those fetuses that survive to the neonatal period, surgical treatment options exist and some success has been reported with the use of postnatal vein embolization, although the mortality for this procedure is around 30%.
Head and neck tumors
The range of head and neck tumors is significant and includes teratoma, lymphangioma, congenital goitre, thyroid or parathyroid tumors, thyroid cysts, neuroblasmtoma or hamartomas. Tumors of the fetal face usually present early with a persistently open fetal mouth even before the development of associated polyhydramnios. Head and neck tumors may grow large enough to cause obstruction of the fetal airway. If inadequately prepared for, this can be both fatal for the fetus and extremely distressing for the attending clinical team. Other potential complications include polyhydramnios and preterm birth secondary to esophageal obstruction, labor dystocia secondary to tumor size, or spontaneous rupture of the tumor leading to fetal death from exsanguination.
Lymphangioma
Cystic hygroma, otherwise called lymphangioma, is a benign malformation of the lymphatic drainage. They can develop anywhere within the body but commonly affect the neck and thorax. Normally, the lymphatic system begins to form at 5 weeks of gestation. Failure of the jugular lymph sacs to join with the lymphatic system leads to the development of progressively enlarging cystic structures on the lateral and posterior aspects of the neck.
Identification of a cystic hygroma in the first or second trimester carries the risk of fetal demise in utero, and also requires discussion of invasive testing as >50% will have an underlying chromosomal disorder and may also have other anomalies. The common associations include Turner syndrome, Down’s syndrome (trisomy 21), Edward’s syndrome (trisomy 18) and Noonan syndrome. Even with a normal karyotype, the risk of major structural anomalies in these fetuses remains high (34%), predominantly cardiac or skeletal[10]. Overall, a normal outcome can be expected in 17% of fetuses diagnosed with a first-trimester cystic hygroma.
Lymphangioma can also present later in the third trimester after normal routine ultrasound examination. These later onset lymphangiomas are usually located on the anterior neck and the prognosis is generally better. They do not appear to have the same association with aneuploidy or coexistent anomalies.
Appearances on ultrasound are of a large cystic mass with multiple septations commonly observed in the posterior triangle of the neck (Figure 13.1). It may be difficult to differentiate increased nuchal translucency from cystic hygroma at early gestations as both may contains septations[11]. Other differential diagnoses need to be excluded by confirming integrity of the skull (posterior encephalocele) and lack of solid or calcified components (teratoma), ascites or pleural effusions (nonimmune hydrops). If there is doubt, fetal MRI may be beneficial to distinguish between cystic hygroma and cervical teratoma (Figure 13.2).
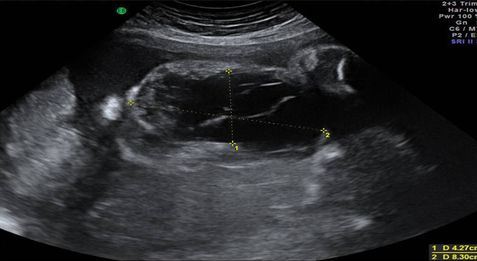
Ultrasound appearance of a large cervical lymphangioma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


