17 Failure to Thrive
Etiology and Pathogenesis
Nonorganic Factors
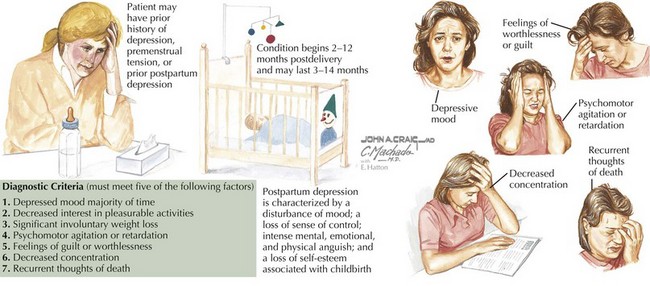
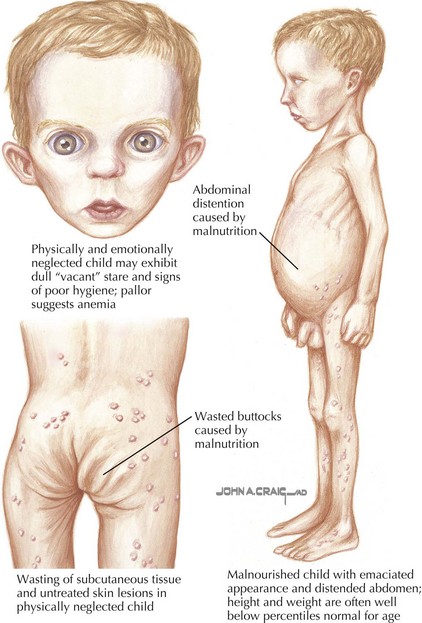
Even if a family is food secure, stressors associated with poverty can cause attachment problems, leading to difficulty in feeding for susceptible children. Families living in shelters or with many family members may have little control over when and where children are fed. Children whose temperaments and appetites require more routine or more frequent meals sometimes fail to thrive in these settings. Domestic violence can be associated with FTT through its detrimental effects on the caregiver, child, or both. Caregiver mental or physical illness, including postpartum depression (Figure 17-1), can also lead to disturbances of attachment. Children who are failing to thrive are at increased risk for abuse and neglect compared with the general population, but most experts believe that the majority of children with FTT are not abused or neglected (Figure 17-2). Some children in stressful living environments appear to have problems absorbing and using calories for growth because they grow poorly despite apparently adequate caloric intake and lack of organic causes for growth failure.
Clinical Presentation
Patients may present throughout infancy and early childhood, although most cases of FTT start in the first year of life. Weight is generally affected earlier and more severely than length. Psychosocial dwarfism is a distinct problem that occurs in patients older than 3 years of age and primarily affects height. Waterlow’s categorization of FTT as mild, moderate, and severe is determined by comparing a child’s growth parameters with the median values for the child’s age and height. Growth patterns demonstrating each of the three classes of FTT are shown in Figure 17-3.
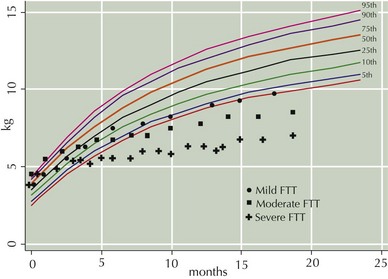
Figure 17-3 Growth chart with points depicting growth patterns of mild, moderate, and severe failure to thrive.
Differential Diagnosis
The differential diagnosis for FTT is broad and often multifactorial. As already noted, many psychosocial stressors and many chronic medical conditions could contribute to FTT. A list of some conditions to consider in the differential diagnosis is presented in Box 17-1.
Box 17-1 Differential Diagnosis of Failure to Thrive
Conditions to Consider



