Fig. 14.1
Bartholin gland and Skene/paraurethral gland duct openings within the vagina
The Vagina
The formation of the vagina starts with the development of two solid sinovaginal bulbs in the superior aspect of the vaginal portion of the urogenital sinus. These bulbs grow distally and form a solid vaginal plate. As the central aspect of the vaginal plate disintegrates, the lumen of the lower vagina is created and completed by 20 weeks. This lower vaginal lumen is separated from the more superior urogenital sinus and uterovaginal canal by the hymenal membrane. This membrane disintegrates centrally before birth, leaving behind a circumferential tissue band within the distal vagina and proximal to the vaginal introitus [2].
Anatomy
Vaginal Structure and Histology
Knowledge of pertinent normal lower genital tract anatomy is also useful when identifying vaginal and vulvar cysts [3]. The vagina, an empty tubular structure with a lumen that is held in place by its surrounding muscular and connective tissue support structures, sits between the bladder and rectum. The most proximal aspect of the vagina, the vaginal apex, heads posteriorly toward the ischial spines. Normal vaginal length is generally between 7 and 10 cm. In the absence of prior total hysterectomy, the cervix is present at the vaginal apex. The outer portion of the cervix (the ectocervix) is made of nonkeratinized stratified squamous cells and the inner portion and canal of the cervix (the endocervix) is comprised of simple columnar cells. Where these two different cell types meet is termed the transformation zone. The vaginal walls consist of three layers. The first layer in direct communication with the vaginal lumen is the vaginal epithelium (also referred to as “mucosa” despite an absence of glands) that is made of nonkeratinized stratified squamous epithelium. Deep to the mucosa is the muscularis that contains smooth muscle, collagen, and elastin. The deepest layer is the adventitia that is made of collagen and elastin connective tissue. The muscularis and adventitia together are referred to as the fibromuscular layer, and is commonly referred to as the pubovesicocervical fascia anterior to the vagina or the rectovaginal fascia posterior to the vagina. On the lateral aspects of the vagina, the adventitia extends out to the pelvic walls and contains fat, lymphatics, and neurovasculature.
Vaginal Neurovasculature
Blood is supplied to the vagina from the descending cervical branch of the uterine artery and branches of the internal iliac artery including the vaginal, middle rectal, and internal pudendal arteries. Lymphatic drainage of the upper two-thirds of the vagina is to the obturator nodes as well as the external and internal iliac nodes, while the lower third of the vagina drains to the inguinal nodes [4]. Portions of the inferior hypogastric plexus are responsible for sympathetic innervation of the vagina [5].
The Urethra
The urethra, which averages 3 cm in length, rests on and is supported by an endopelvic fascial layer and the anterior vaginal wall [6, 7]. It is comprised of four layers: mucosa, submucosa, internal urethral sphincter made of smooth muscle, and striated external urethral sphincter made of skeletal muscle. The inner surface of the proximal urethra is lined by transitional epithelium while the distal urethra is lined by stratified squamous epithelium [8]. This epithelium is continuous with bladder epithelium proximally and with that of the vaginal vestibule distally. Paraurethral glands open into the urethral lumen within this layer in the dorsal or vaginal side of the distal urethra [9]. The most pronounced of these paraurethral glands are the Skene glands that can be visible on the inner surface of the external urethral meatus. Blood supply to the urethra comes from the internal pudendal, vaginal, and inferior vesical arteries, while nerve supply comes from the pudendal nerve for somatic control and portions of the inferior hypogastric plexus for autonomic control [10]. The lymphatics of the distal third of the urethra drain into the superficial or deep inguinal nodes, whereas the proximal two-thirds drain into the external iliac, internal iliac, and obturator nodes.
The Vulva
The vulva is the term for the female external genitalia and includes the mons pubis, labia majora, labia minora, clitoris, vestibule, vestibular bulbs, vestibular glands, Bartholin (greater vestibular) glands, Skene (paraurethral) glands, external urethral meatus, and vaginal orifice. The skin over the mons pubis and labia majora has hair and a fatty subcutaneous layer. The obliterated processus vaginalis, or canal of Nuck, and the round ligament exit the inguinal canal and terminate within the fat or skin of the labia majora. The skin over the labia minora does not have hair and its subcutaneous tissue is devoid of fat.
The vaginal vestibule is an area in between the labia minora. The specific boundaries include the clitoris anteriorly, the fourchette posteriorly, the Hart line laterally, and the hymen medially. Distal to the Hart line the exposed tissue is a keratinized stratified squamous epithelium, while proximally it is nonkeratinized stratified squamous epithelium. The vestibule also contains the urethral, vestibular, Bartholin, and Skene gland openings.
The Bartholin glands are the female equivalent of the male bulbourethral, or Cowper, glands. One gland is situated at 5 O’clock while the other rests at the 7 O’clock position and each gland possesses a duct that opens into the vaginal vestibule. The inner surfaces of these glands are lined by columnar cells that secrete mucus to provide lubrication [11].
Evaluation and Management
History and Physical
A history and physical exam is the starting point of any vaginal or vulvar cyst workup. Specific symptoms to address in the patient’s history of present illness include the presence or absence of vaginal or vulvar pain, dyspareunia, urethral versus vaginal discharge, spotting, post-void dribbling, leakage of urine, dysuria, incomplete voiding, or palpable mass. The patient should be questioned regarding recent vaginal trauma or placement of foreign body into the vagina. Pertinent aspects in the history include age, known congenital urogenital tract anomalies, obstetrical history including vaginal trauma and repair, sexual activity, recurrent urinary tract infections, prior vaginal surgery, and history of pelvic radiation therapy. Gynecological history including menstrual cycles, prior vaginal infections, endometriosis, fibroids, and exposure to diethylstilbestrol (DES) in utero may be specifically applicable to the patient’s presenting condition.
A targeted physical examination should include bimanual and speculum exams. A pelvic organ prolapse assessment to rule out prolapse as a cause for vaginal bulge symptomatology should be completed. Special attention should be taken to palpation of the anterior vaginal wall; a compressible bulge and discharge per urethra should raise suspicion for urethral diverticulum. Vaginal discharge should be evaluated. Masses such as cystic-appearing bulges should be examined with special attention taken to note the size, location, and tenderness of the cyst.
Differential Diagnosis
Vaginal Cysts
The differential diagnosis of vaginal cysts (Table 14.1) includes epidermal inclusion cysts, mullerian cysts, Gartner duct cysts (mesonephric remnants), and mucous inclusions (adenosis). Less common types of vaginal cysts include endometriotic cysts and vaginitis emphysematosum. Vaginal endometriotic cysts are infrequently encountered as the vagina is a rare location for endometriotic implants to manifest [12]. Although the etiology remains unclear, the benign and self-limited condition of multiple gas-filled cysts lining the vaginal wall (vaginitis emphysematosum) has also been described [13].
Table 14.1
Differential diagnosis of vaginal and vulvar cysts
Vaginal cyst | Vulvar cyst |
|---|---|
Epidermal inclusion cyst | Epidermal inclusion (sebaceous) cyst |
Mullerian cyst | Bartholin (greater vestibular) gland cyst |
Gartner duct cyst (mesonephric remnant) | Skene (paraurethral) gland cyst |
Adenosis (mucous inclusions) | Cyst of the canal of Nuck (hydrocele) |
Endometriotic cyst | Leiomyoma |
Vaginitis emphysematosum | Urethral diverticulum |
Vulvar Cysts
The differential diagnosis of vulvar cysts (Table 14.1) includes vulvar epidermal inclusion (sebaceous) cysts, Bartholin (greater vestibular) gland cysts, Skene (paraurethral) gland cysts, cysts of the canal of Nuck (hydroceles), leiomyoma, and urethral diverticulum (Fig. 14.2; see Chap. 11 on Repair of Urethral Diverticula).

Fig. 14.2
Urethral diverticulum
Overall, the frequency of presentation with a vaginal cyst is uncommon. Patients are more likely to present with symptomatic vulvar cysts. Kondi-Pafiti et al. [14] reviewed 40 cases of benign vulvar and vaginal cysts, the majority of which were asymptomatic. The most common symptomatic cyst was a Bartholin gland cyst. The most frequently encountered cyst was a mullerian cyst (12), followed by a Bartholin gland cyst (11), epidermal inclusion cyst (10), Gartner’s duct cyst (5), endometrioid cyst (1), and one unspecified cyst. Deppisch [15] studied the classification of 64 surgically excised vaginal cysts and found that Gartner’s duct cysts were uncommon, mullerian cysts made up 1/3 of cases, and epithelial inclusion cysts were the most common type of vaginal cyst. These studies are consistent with the general acceptance that epithelial inclusion cysts, mullerian cysts, and Bartholin gland cysts more often cause symptoms and are therefore more likely identified than other types of vulvar or vaginal cysts.
Evaluation of Vaginal Cysts
Epidermal Inclusion Cysts
Epidermal inclusion cysts are often asymptomatic and discovered during routine gynecological exam. However, symptoms may include vaginal pain or dyspareunia and presence of a palpable mass. The appearance is round, pinkish-white in color, and variable in size (Figs. 14.3, 14.4, 14.5, and 14.6). The fluid content can be viscous. Histopathology confirms the diagnosis and reveals epithelial cells lined by a cyst wall made of nonkeratinized stratified squamous epithelium. Asymptomatic cysts can be observed, while drainage or excision should be performed for symptomatic cysts or if there is concern for infection. Additionally, the cyst should be biopsied and drained or excised for patients with a history of cervical, vaginal, or vulvar intraepithelial neoplasia. Hoffman et al. [16] reported on 26 women who were treated for vaginal intraepithelial neoplasia, 22 of whom had undergone prior hysterectomy for benign causes, cervical intraepithelial neoplasia, or malignancy. Five patients were noted to have vaginal cuff inclusion cysts that were found to be positive for a neoplastic process. This finding suggests that when a vaginal epithelial inclusion cyst is identified in a patient with a prior intraepithelial neoplastic process or cancer, biopsy of the cyst should be performed.
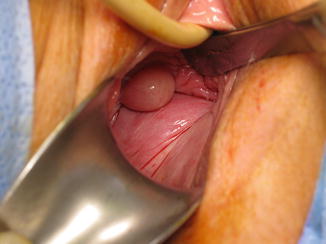
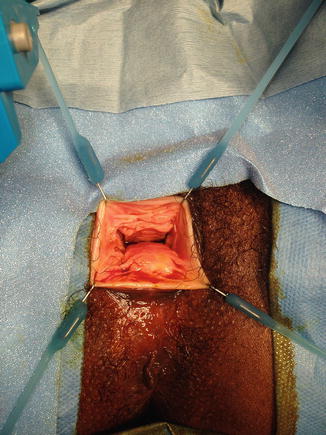

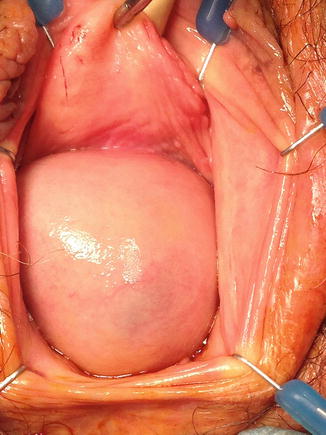
Fig. 14.3
Epidermal inclusion cyst arising from right lateral vaginal wall
Fig. 14.4
Epidermal inclusion cyst arising from posterior vaginal wall
Fig. 14.5
Epidermal inclusion cyst (visually difficult to distinguish from pelvic organ prolapse)
Fig. 14.6
Showing base of epidermal inclusion cyst shown in Fig. 14.4 arising from mid-portion of anterior vaginal wall
Gartner Duct Cysts
On physical exam these cysts are typically identified within a lateral wall of the vagina. Gartner duct cysts are mesonephric (Wolffian) duct remnants. During embryonic development the mesonephric ducts are involved in the formation of the urogenital system. In females, after the fundamental urinary system is created, these ducts regress and sometimes leave a remnant behind causing a Gartner duct cyst. They are usually asymptomatic and encountered during routine gynecological exam. When present, symptoms include vaginal pain, dyspareunia, or the awareness of the presence of a mass. Histologically, they are lined with cuboidal or columnar epithelium. Asymptomatic cysts can be observed while symptomatic ones should be marsupialized or excised. If surgical management is pursued, it is important to image the lower reproductive tract because Gartner duct cysts can track cephalad as far as into the broad ligament and an awareness of the cyst dimensions may prove helpful during dissection (Figs. 14.7 and 14.8). Furthermore, imaging is performed to detect renal anomalies with which Gartner duct cysts may be associated [17]. Bats et al. [18] reported a case of malignant transformation of a Gartner cyst in a 67-year-old woman who presented with vaginal bleeding. Pathology from excision revealed clear cell carcinoma. Although the risk of developing carcinoma from a Gartner duct cyst is extremely rare, we suggest performing at least a biopsy if not an excision in patients with vaginal bleeding.
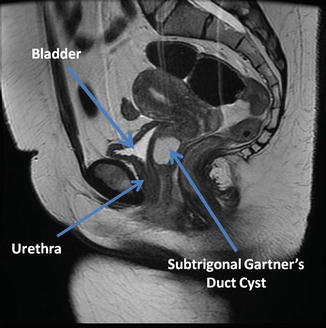
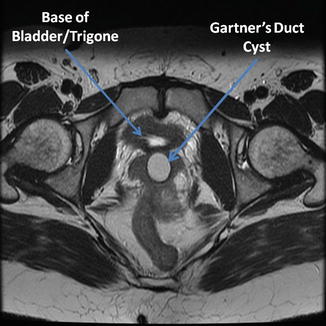
Fig. 14.7
MRI sagittal view of Gartner duct cyst (Courtesy of Howard Goldman, MD, Department of Urology, Cleveland Clinic, Cleveland, OH)
Fig. 14.8
MRI transverse view of Gartner duct cyst (Courtesy of Howard Goldman, MD, Department of Urology, Cleveland Clinic, Cleveland, OH)
Adenosis
Vaginal adenosis is a condition where mucous inclusions (glandular tissue) are present within the vaginal epithelium. The etiology can be spontaneous, but many affected patients were exposed to diethylstilbestrol (DES) in utero. Symptoms include vaginal discharge, irritation, pruritis, dyspareunia, and postcoital spotting. The area of affected vaginal wall appears erythematous and grainy or possibly with multiple small (millimeter) cysts. Histology displays normal vaginal stratified squamous mucosa containing regions of columnar epithelium. Those patients with a history of DES exposure are at increased risk for developing vaginal clear cell adenocarcinoma. Because of the risk of underlying carcinoma, a colposcopic exam should be performed with biopsy. The condition is usually self-limited; however, if persistent or symptomatic, treatment with carbon dioxide laser coagulation or excision can be considered. See Fig. 14.9a, b.
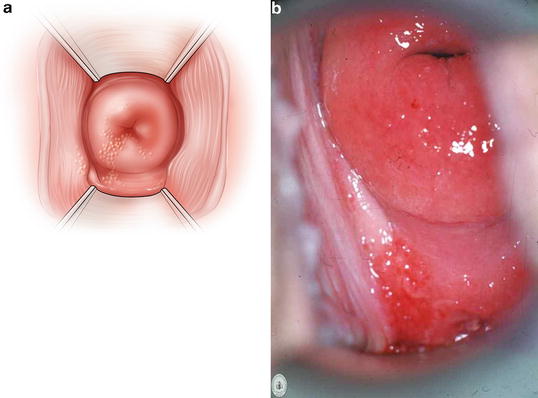
Fig. 14.9
(a, b) Vaginal adenosis
Vaginitis Emphysematosum
Vaginitis emphysematosum is an uncommon abnormality that produces multiple subcentimeter gas-filled cysts within small connective tissue spaces in the vaginal wall giving it a corrugated appearance. As reported by Leder et al. [19] the etiology of this benign bacterial vaginitis is uncertain, but most reported cases have noted the presence of vaginitis caused by Trichomonas vaginalis or Gardnerella vaginalis. The condition is often discovered in gravid or immunocompromised patients and usually does not cause symptoms. When present, symptoms may include vaginal discharge and pruritis. The condition can be observed on imaging such as X-ray or Computed Tomography (CT) scan. Histology reveals gas spaces beneath the vaginal epithelial pegs that are lined by inflammatory multinucleated giant cells. Vaginitis emphysematosum is benign and self-limiting.
Mullerian Cysts
As most vaginal cysts, mullerian cysts are most often asymptomatic and found on incidental exam. However, symptoms may include dyspareunia and presence of a palpable mass detected either manually or while attempting to insert a tampon. They appear round, smooth, pink, variable in size, and fluid content feels gelatinous when palpated. On exam, it is not possible to distinguish mullerian cysts from inclusion or Gartner’s duct cysts. Histology reveals a columnar epithelial lining. Once again, asymptomatic cysts can be observed whereas incision and drainage or excision should be performed for symptomatic or infected cysts. There have been several case reports documenting vaginal mullerian cysts. In one report, a woman presented with an 8 cm posterior vaginal wall cyst that contained mucoid material [20], while another case reported a large anterior vaginal wall cyst that was evaluated with radiologic studies and subsequently excised [21]. There has been one unusual report of adenocarcinoma arising from a vaginal mullerian cyst in a 48-year-old presenting with a 3 cm ruptured vaginal cyst [22]. This finding highlights the need to have a low threshold for biopsy when larger or persistent anatomical abnormalities are encountered.
Imaging
The role of radiography in evaluation of a vaginal cyst depends on the location and type of cyst suspected after performing a history and physical exam. Based on the initial evaluation, it may be prudent to obtain preoperative information regarding cyst characteristics and its proximity to neighboring structures. For example, Gartner duct cysts (mesonephric remnants) may extend as far cranially as into the broad ligament and preoperative imaging may help determine the extent of intraoperative dissection that will be necessary. Additionally, since Gartner duct cysts can be associated with renal anomalies, preoperative imaging may expose findings such as renal agenesis or ectopic ureter. Sheih et al. [23] found 13 cases of cysts in the pelvis that were associated with ipsilateral renal agenesis or dysplasia after 280,000 children with renal abnormalities were screened with ultrasounds. Seven of the 13 cases found to have pelvic cysts were girls with Gartner duct cysts.
Preoperative imaging may be useful in identifying additional cysts that were not visible on physical exam. Wai et al. [24] reported a case of a 20-year-old woman who presented with two vaginal cysts on exam. Magnetic Resonance Imaging (MRI) was obtained preoperatively and not only demarcated the arrangement of her vaginal cysts, but also identified additional larger cysts that had not been appreciated on physical examination.
Evaluation of Vulvar Cysts
Vulvar Epidermal Inclusion Cysts
Vulvar epidermal inclusion cysts, also known as sebaceous cysts, are the most common vulvar cysts. They form on areas where hair follicles or sebaceous glands are present. Additionally, clitoral epidermal inclusion cysts have been described in patients with a history of female genital mutilation. Rouzi et al. [25] reported on 21 females presenting anywhere between 2 and 20 years after having had a type I female genital mutilation procedure, whereas Ofodile et al. [26] described 19 cases. Most vulvar inclusion cysts are asymptomatic. When present, symptoms include pain to touch and bothersome appearance. These cysts appear firm, are often mobile, and contain caseous material. They run the risk of becoming infected and developing into cellulitis or an abscess. Obstruction of the duct leads to buildup of secretions and consequently cyst formation. Treatment includes warm compresses to drain the obstructed duct. Recurrent, persistent, or enlarging cysts can be treated with incision and drainage, punch biopsy with subsequent drainage, or excision. The type of excision may depend on the cyst size (to be described later in the chapter). In a randomized prospective study of 60 patients with nonspecifically located noninfected vulvar epidermal inclusion cysts, Lee et al. [27] compared results after treatment with the punch biopsy technique versus excision. The study group found that those treated with the punch biopsy method produced superior cosmetic results, while there was no difference in recurrence rates over the 16-month time period they were studied.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


