CHAPTER 9 Esophageal Replacement
Gastric Tube Pull-up
Step 1: Surgical Anatomy
♦ Esophageal atresia remains the most common reason for esophageal replacement in children. The stomach will usually have a normal configuration and, in cases of pure esophageal atresia, will have a gastrostomy tube in place at the time of esophageal replacement. The stomach in pure atresia is diminutive at birth and requires several months of feedings before attaining a normal size.
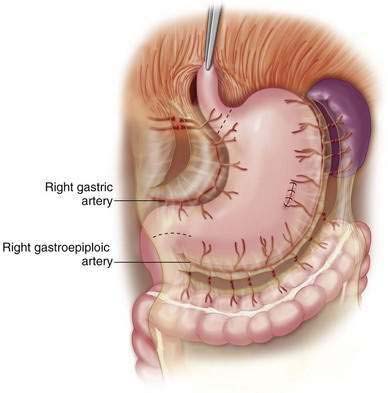
♦ A key element of the anatomy is the blood supply to the stomach. The transposed stomach will rely on the right gastric and the right gastroepiploic arteries, which must be preserved (Fig. 9-1).
♦ The left gastric and the short gastric arteries are ligated to mobilize the stomach. It is prudent to temporarily occlude flow to the left gastric artery using a bulldog clamp before ligation to ensure that the stomach will have adequate perfusion from the remaining vessels. If the perfusion appears inadequate, an alternate esophageal substitution is required.
♦ Another important anatomic point is that the most cephalad portion of the stomach will be the fundus, not the gastroesophageal junction (GEJ).
♦ In cases of atresia, the esophageal bed will be without scarring or adhesions unless previous attempts at repair have been made. Significant scar formation may be present in children with severe caustic injury to the esophagus and in cases where there is a history of perforation or prior attempts at a replacement procedure.
♦ In some cases, a cervical esophagostomy may be present at the time of surgery. This will usually be on the left side of the lower neck, which is more desirable because the path through the mediastinum is shorter to this side. It is critical to be aware of the vagus and the recurrent laryngeal nerves at the time of surgery. Both recurrent laryngeal nerves can be injured and will result in severe respiratory compromise because of vocal cord paralysis.
Step 2. Preoperative Considerations
♦ We recommend preoperative admission for bowel preparation in case the stomach is not usable for esophageal replacement and the colon is required.
♦ Children with a history of atresia may have concomitant cardiac defects and should have a cardiology workup done as needed.



