18
Ear, nose and throat
Chapter map
ENT problems are very common in children. The upper respiratory tract is the most common site of infection in the young child, and assessment of acute illness is not complete without examination of the ears, nose and throat (Section 3.5.2). Chronic disorders are important causes of long-term morbidity. The early diagnosis of sensorineural and conductive hearing loss is essential if educational and social effects are to be minimized (Section 10.4.5). Often more serious or chronic disorders are managed together with a paediatric ENT surgeon.
18.1.2 Otitis media with effusion (glue ear, secretory otitis media)
18.1 Ear problems
18.1.1 Otitis media
Acute otitis media is common throughout the first 8 years. In the older child, the cardinal symptom, ear ache, makes detection easy; in infants it may not be so obvious. They usually have high fever and are irritable, rolling their heads from side to side, or rubbing their ears. Initially there is mild inflammation of the pars flaccida (the superior part of the tympanic membrane) with dilated vessels running down the handle of the malleus, and an absent light reflex. This progresses to a red, bulging, painful tympanic membrane, perforation and discharge of pus. A mildly pink dull drum may be present in any URTI.
A majority of otitis media is viral, but distinction from bacterial infection is difficult. The evidence indicates that simple analgesia is all that is needed in most cases, but antibiotics (amoxicillin) should be given if the child is very unwell, vulnerable (e.g. through immunosuppression or prematurity) or if symptoms persist for more than 4 days. Paracetamol is invaluable for the fever and pain. Persistent aural discharge (chronic suppurative otitis media) is a potential complication. To prevent further episodes, ensure pneumococcal immunizations are up to date, and avoid passive smoking, dummies (pacifiers), and supine feeding.
- Mastoiditis
- Lateral sinus thrombosis
- Meningitis
- Cerebral abscess.
18.1.2 Otitis media with effusion (glue ear, secretory otitis media)
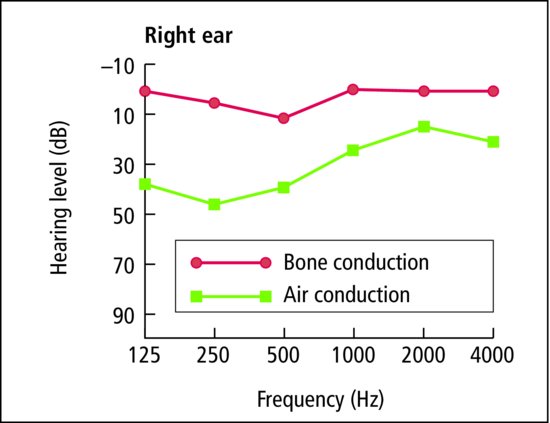
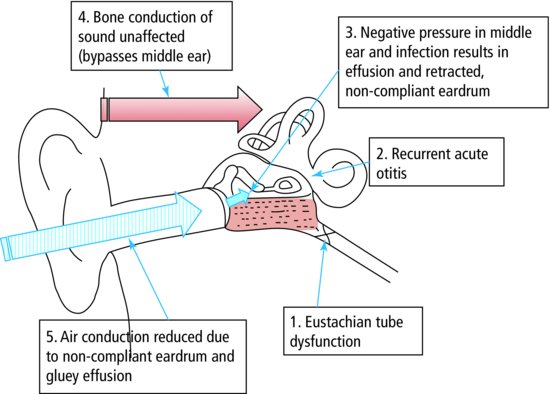
Glue ear is the most common cause of conductive hearing loss below the age of 10 years (Figures 18.1, 18.2 and 18.3). Sticky, serous material accumulates in the middle ear insidiously or after acute otitis media. The symptoms are deafness, speech delay, and older children may report a feeling of fullness or popping in the ear. It is especially common in children who have atopy, frequent upper respiratory infections or cleft palate. The eardrum is usually dull and retracted, and a fluid level may be seen. The malleus handle is more horizontal and appears shorter, broader and whiter. Antibiotics, antihistamines and decongestants may be tried. If there is significant deafness, an indwelling tube (grommet) is inserted through the eardrum to aerate the middle ear and is left for 6–12 months.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


