23 Ear and Nose Problems The following case of recurrent ear infections is of a young boy who came for treatment before I had learned Meridian Therapy sufficiently well to apply it on children. Thus, besides some simple symptomatic treatment, the principle treatment was the core non-pattern-based root treatment that is typical of the shonishin system. This case is selected as it is typical of what happens when treating children with recurrent ear infections. Of course, treatment does not always work as well and smoothly as this, hence more detailed treatment options are also given below, but Mike was the first of a number of 3–6-year-old children that I treated for recurrent infections as Mike’s parents were in a position to get the word out and refer other children. Case 1 Main complaints: Mike came for treatment having just completed a round of antibiotics for infections in both ears. The right ear had, as usual, been much worse than the left ear. Over the last 10 months he had had many ear infections. With each, the doctor eventually prescribed antibiotics, which would clear up the episode, but within 2 weeks of completing the antibiotics another infection would start, sometimes only in the right ear, but often in both. The problem had started initially from catching a bad cold and having it progress to the ears, but since then, while several episodes of ear infection had arisen from catching cold, many had not. He had been very disrupted by this process as the pain would often be bad and would disturb sleep, energy, and the rest of the family. The antibiotics disturbed his digestion a bit, with some episodes of loose stools and some episodes of constipation. The parents were interested in trying something different, as it was clear that the problem was not going away; rather, it was being suppressed by each round of antibiotics. The doctor had recently said that if this kept up Mike would probably have to have ear tubes placed to help prevent further problems. The parents were looking for a treatment to break the cycle of infections. Other than the problem of recurrent ear infections Mike was healthy and all other systems were unremarkable. Assessment: Palpation revealed hard painful areas below each ear extending downward from TB-17, the right being more hard and uncomfortable than the left. The occipital border was also stiff, especially around GB-12. Treatment: On this first visit I decided to apply a shonishin core treatment with light stroking and some targeted tapping. Light stroking with an enshin was applied down the arms (three yang channels), legs (stomach, gallbladder, and bladder channels), down the back, across the shoulders, chest, and down the abdomen (stomach channel). Light tapping was applied above and behind both ears, and over the reactive regions below the ears and over the occipital region, especially around GB-12. Press-spheres were placed at GV-12 and on the most reactive point within the reactive regions below each ear. I discussed with the parents that it would be ideal to give treatment more than once a week to increase the chances of preventing recurrence of the infections, but they told me as working parents they were too busy to be able to do this. So I told them I would figure out what to do about it. Second visit—1 week later Mike was doing well, there were no signs of ear infection, nothing to report. Treatment: A very slightly increased dose of the same treatment as given on the first occasion was applied. I then proceeded to explain to the parents how to do the light stroking and tapping treatment at a low dose each day: stroking down the same areas on the arms, legs, back, shoulders, and tapping on the areas around the ears and GB-12 region. Mike was still fine, with no sign of an infection. The home treatments had been going well and took about 2–3 minutes each day. Treatment: The same treatment as given on the first occasion was applied. Fourth visit—1 week later Still nothing to report, Mike had no symptoms. Home treatment was going well. Treatment: The same treatment as given on the first occasion was applied. I also scheduled Mike to come back in 2 weeks to stretch out treatments while the parents continued doing daily home treatment. Fifth visit—2 weeks later Still nothing to report, Mike had no symptoms. Home treatment was going well. Treatment: The same treatment as given on the first occasion was applied. Sixth visit—2 weeks later Still nothing to report, Mike had no symptoms. Home treatment was going well. Treatment: The same treatment as given on the first occasion was applied. We now extended treatment to every 4 weeks. Seventh visit—4 weeks later Still nothing to report, Mike had no symptoms. He had caught cold and for the first time it did not trigger an ear infection and he recovered from the cold quickly. Treatment: The same treatment as given on the first occasion was applied. Eighth visit—4 weeks later Still nothing to report, Mike had no symptoms. Home treatment was going well. Treatment: The same treatment as given on the first occasion was applied. After this we stopped treatment. Mike had had no sign of an ear infection for about 4 months; it looked like we had broken the cycle. The parents were still applying the simple home treatment regularly but without the press-spheres. They agreed to call for treatment should Mike start an ear infection. At another 4-month follow-up conversation, Mike was still fine. He seemed to catch cold less often than before and had no sign of any further ear infections. His parents referred many other children with ear infections for treatment. Our aim is to improve the overall condition of the child so he or she has better resistance to infections and treat to deal with the local manifestations that additionally make the child susceptible to ear infections. Changing the overall condition of the child can be accomplished with just the use of the basic core shonishin treatment or the pattern-based root treatment, but it generally works better if you apply a combination of these two treatment approaches. If the recurrent ear infections arise from catching cold repeatedly, the typical pattern to be treated is the lung vacuity pattern. If the ear infections arise independently of catching cold, this could be due to lung vacuity pattern or kidney vacuity pattern. If the child is young and the pulse and other signs for distinguishing the pattern are not clear, one needs other signs to distinguish them. If the hands tend to be cold, it is likely to be a lung vacuity pattern and one should start treating this. Having generally stiff shoulders is also a sign of lung vacuity type. However, if the feet tend to get cold easily (but not the hands) this is more likely to be a kidney vacuity pattern. You may also notice some small temperature variations on the abdomen to support the choice of kidney pattern, such as slightly cooler below the navel compared with above the navel. Also, if the ear infections have triggered changes in hearing, you can suspect the kidney vacuity pattern. Case 2 below illustrates an alternative strategy for treating the relevant acupoints, using a very light stroking along the flow of the channels over the target acupoints for supplementation, and light stroking against the flow of the channel over the target acupoint for draining. One can apply either the core non-pattern-based treatment with stroking and some tapping or tapping alone. For treatment apply stroking down the arms, legs, back, and abdomen. If the shoulders are stiff, apply stroking across the shoulders. If the neck is stiff, apply stroking down the neck. Apply tapping to around GV-12 (see Fig. 23.1). It has been my consistent experience that children with otitis media develop an area of stiffness that is usually painful on pressure below the ears. This hardened area usually starts around TB-17 and extends downward from there. Sometimes it extends backward from there towards GB-12, sometimes forward slightly from there. I feel that this area of stiffness is probably associated with blockage of the lymphatic drainage, and that it is thus an important area to target. Thus, I always apply tapping to this area as well as the areas above and below the ears that are suggested by Yoneyama and Mori (1964) and Hyodo (1986). I give a consistent focus to soften and break up this congested, hardened area. If the tapping alone does not make enough change I start applying stronger techniques to it such as press-spheres, needling, and/or press-tack needles. See below. Fig. 23.1a, b Usual stroking plus: • Below, above, and behind the ear(s): 10 times each • Occipital area: 10 to 20 times • Across the shoulders: 10 to 20 times • GV-20 area: 10 to 20 times • GV-12 area: 10 to 20 times • LI-4: 10 to 20 each • ST-12 area (supraclavicular fossa region): five to 10 times each Whether one inserts needles and immediately removes them or inserts and retains them for a short while, needling can be helpful in the treatment of otitis media. The area of hardness and pressure pain below the ears can be a useful place to needle. The area around GB-12 can also become stiff and reactive, and this responds well to light needling. It is useful to leave press-spheres on the hardened sensitive area(s) below the ear(s). If these areas do not sufficiently change I recommend switching soon to a stronger technique such as leaving press-tack needles and maybe needling during the session. In order to help the child settle (ear infections can be quite painful and distressing) it can be helpful to also leave a press-sphere on GV-12. The main area for leaving the small press-tack needles (0.3mm or 0.6 mm long) is the area below the ear(s), around TB-17 or below that point. On older children, where it is generally safer to leave intra-dermal needles, I leave them at the stubbornly reactive points such as the area of reaction below the ears. The application of small direct moxa cones is recommended at points such as KI-2, KI-3, with KI-2 being especially effective (Yoneyama and Mori 1964). The following points are recommended on adults; they can be palpated and the most reactive one or two points treated with moxa for non-responsive otitis media (KI-3 is strongly recommended): SI-19, TW-17, GB-12, HT-3, KI-3, BL-23, BL-11, BL-12 (Shiroda 1986). If you are afraid to moxa these points because it is too difficult you can try applying needling, press-spheres, press-tacks, or intra-dermal needles to the reactive points from this list (keeping in mind the issue of dose of treatment). Cupping can be helpful over the upper back and backs of the shoulders to help get the area to relax when chronically stiff in the child with recurrent otitis media. As discussed in Chapter 14, be careful about the dose; applying the cups repeatedly for less time can be helpful. Bloodletting of the jing point GB-44 is recommended for ear pain (Birch and Ida 1998, p. 240), TB-1 could also be indicated (Birch and Ida 1998, p. 283). It can be very difficult to apply this technique on small children, and even on older children. You must have a painless technique. If the child with recurrent otitis media shows vascular spiders on the upper back in the GV-14 area or back of the shoulders, it can on occasion be useful to apply vascular spider bloodletting. This is usually easier to do than jing point bloodletting on a child, but your technique must be very good; otherwise do not apply it. If you do this, apply only the stabbing and squeezing method; do not also apply cupping. You might choose to try the bloodletting because the child’s problem is not changing and you have already tried other stronger techniques such as needling or direct moxa. As discussed in Chapter 15, it will be important to make sure that the child will stay still for you and that you have a clear agreement with the child’s parent to proceed. It can be a good idea to examine the diet of the child. Often with repeat infections, cow’s milk products can be an irritant. Testing for and stopping the intake of cow’s milk products can be important for some children, and so I always check this out. It is wonderful to have parents who have children with repeated infections start to apply treatment at home. It not only makes the overall treatment more effective, but gives the parents a sense of being able to help and contribute. The following case is from the practice of my colleague Zoe Brenner in Bethesda, Maryland, United States. Case 2 The mother had been a long-time patient and mentioned that her 4-year-old was having chronic ear infections, resulting in difficult speech development because her hearing was impaired. She wanted to bring her in for treatment. Diagnosis: Both the fact that she had ear problems with hearing difficulties and that she exhibited so much fear suggested the kidney vacuity pattern. First visit When the mother brought Clare, she hid behind her mother. She seemed disproportionately fearful. Treatment: It was not possible to take her pulses that first time. With gentle coaxing it was possible to lightly stroke with the enshin down her legs on the yang channels and up on the yin channels then down her arms on both the yin and yang channels.1 Light stroking with the enshin was also given down her back, stroking through her clothes as she would not remove them. She was a bit more relaxed but still quite wary. __________________ Second visit—1 week later Clare’s mother reported that she had been very happy after the previous visit. Treatment: The same enshin light-stroking core non-pattern-based root treatment was applied. After this she was less fearful and it was possible to take her pulses. The kidney pulse was quite weak with relative repletion on her spleen pulse. To treat this, light treatment was applied using an enshin by stroking along the kidney channel near KI-3. After rechecking the pulses, the spleen pulse was still replete, so gentle stroking was applied against the flow of the spleen channel over SP-9. Third visit—1 week later Clare had been doing well, no problems. Her mother said that the speech therapist noticed that her enunciation was getting clearer and her hearing had improved 20 dB. Treatment: The treatment from the second visit was repeated with the exception that gentle stroking with the teishin in the direction of flow of the lung channel over LU-9 was added after treating KI-3. Fourth visit—1 week later She had mild cold symptoms (runny nose, mild cough), otherwise no ear problems. Her mother was excited to report that Clare had gone to a party and did not hide for the first hour. This was a huge change for her to go in and be able to engage in play right away. Treatment: The same treatment as on the third visit was repeated with the exception of adding a mild pressing over the cheeks and neck below the ears to promote drainage and help with recovery from the cold. Treatment was continued for a few more sessions, spreading them apart more as she continued to improve. The issue with the chronic ear infections, hearing, and speech completely resolved. One of the key signs that she was better came when she had a streptococcus infection affecting the throat with no ear involvement at all. Additionally, her fearfulness was quite improved, as everyone noted.
Otitis Media—Ear Infections
Mike, Boy Age 3½ Years
 General Approach for the Treatment of Otitis Media
General Approach for the Treatment of Otitis Media
 Most Likely Pattern-based Root Diagnosis
Most Likely Pattern-based Root Diagnosis
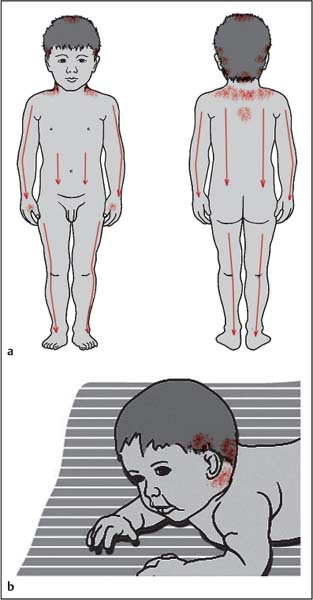
 Typical Non-pattern-based Root Treatment
Typical Non-pattern-based Root Treatment
Additional Areas for Treatment
 Recommendations for Symptomatic Treatment
Recommendations for Symptomatic Treatment
Needling
Press-spheres (Ryu), Press-tack Needles (Empishin), and Intra-dermal Needles (Hinaishin)
Okyu—Direct Moxa
Cupping
Bloodletting
 Other Considerations
Other Considerations
Dietary
Home Treatment
 Further Case Histories
Further Case Histories
Clare, Girl Age 4 Years
Ear and Nose Problems
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


