23 Disorders of the Hip and Lower Extremity
Congenital
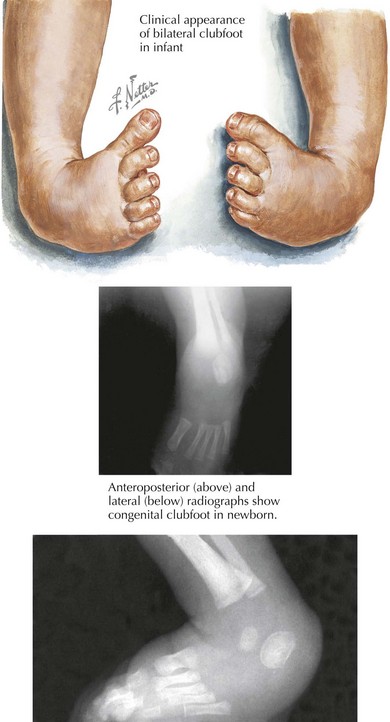
Clubfoot
Clubfoot, or talipes equinovarus, affects one in 1000 live births and is often diagnosed in utero. The condition is characterized by a smaller foot on the affected side, rigidity to plantar flexion, adductus of the forefoot, and inward angulation of the hindfoot (Figure 23-1). Half of cases are bilateral. Although many cases are idiopathic, maternal smoking, certain ethnic backgrounds, and genes affecting both the musculoskeletal and nervous systems have been identified as risk factors. Some believe that disordered development of the talus in utero causes the disorder.
Developmental
In-toeing
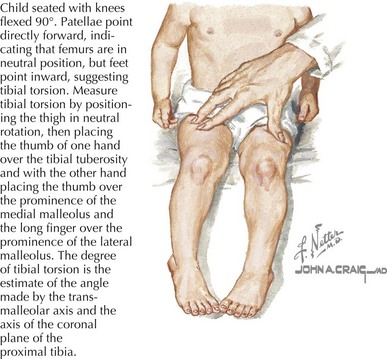
Internal Tibial Torsion
Internal tibial torsion is the most common cause of in-toeing and can be associated with metatarsus adductus. It is usually noted in toddlerhood when children begin to walk. It affects boys and girls equally and is bilateral in about two-thirds of cases. On examination, the knee remains in neutral position while the foot is medially rotated (Figure 23-2). Most cases self-resolve as children begin to walk independently, with normal alignment noted as early as 4 years or as late as 10 years of age.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


