20 Digestive Problems Case 1 Main complaints: Severe problems with constipation since being a baby. Very hard stools; she only passed small quantities at a time as it was painful to pass the stools. She was afraid to go to the toilet because of this pain. Additionally, she had had a lot of intestinal-abdominal pain since birth. She tended to wake every night between 2 and 3 a.m. with this pain. Additional complaints: Hernia of the navel; occasional small patches of dry and itchy skin; variable appetite. All other systems were unremarkable. Diagnosis: From symptoms and pulse: lung vacuity pattern. Treatment: Tapping with the herabari was applied on the abdomen, chest, back, arms, legs, and especially around GV-12, GV-4, and GV-20. Using the teishin, supplementation was applied to right LU-9 and SP-6 (SP-3 and SP-5 were too ticklish). Press-spheres applied and retained on GV-12 and bilateral BL-25 (they were not retained on ST-25 for fear that she might play with or interfere with them). Second visit—2 weeks later The stools had been larger and easier over the 2 weeks, but were still a bit hard. Treatment: Tapping with a herabari was applied on the abdomen, back, arms, legs, around GV-4 and GV-12. Using a teishin, right LU-9 and SP-5 (SP-3 still too ticklish) were supplemented, left LR-3 drained. Press-spheres were placed on GV-12 and bilateral BL-25. The mother was taught to do basic tapping at home daily. Third visit—3 weeks later The stools had been much better, much softer and larger. In the last few days they had become slightly harder again, but there was no more waking at night with pain and no more fear of going to the toilet. Mother and child enjoyed daily home treatments. Treatment: Using a herabari, tapping was applied to the abdomen, back, arms, legs, neck, GV-12 and GV-4 area. Using a teishin, right LU-9 and SP-3 were supplemented, left LR-3 drained. Press-spheres were placed on GV-12 and bilateral BL-25. Fourth visit—4 weeks later Bowel movements were normal, with some variation in frequency (not always daily). No more abdominal pain, still no fear of going to the toilet and no constipation. Treatment: Using a herabari, tapping was applied to the abdomen, back, arms, legs, neck, GV-12, and GV-4 area. Using a teishin, right LU-9 and SP-3 were supplemented, left LR-3 drained. Press-spheres were applied to GV-12 and bilateral BL-25. For financial reasons and because of good progress, treatment was stopped. Daily bowel movements may be an ideal concept but for some people bowel movements at a frequency less than daily can be “normal.” It is important to consider what the parent means by “constipation.” If the child generally has difficulty passing stools such that the frequency is less than daily and causes some distress to the child, giving pain on evacuation, great strain trying to evacuate or fear of going to the toilet, this certainly qualifies and should be treated as constipation. But the child who passes stools without effort four to five times a week and with no associated issues may well be “normal.” You may need to pay attention to the secondary symptoms that accompany the constipation. The young child who is afraid to go to the toilet: is that because it has been painful and the child is afraid of that pain on straining to evacuate? Is it that the child usually feels the urge to evacuate after breakfast when he or she is typically at school and afraid of the more public toilets of the school or does not like using them for bowel movements? The first will usually improve once the child starts more easily passing stools. The second may need more attention as you think about how to help the child feel less nervous. Is this second category more related to a “kanmushisho”-type manifestation? How in general is the child’s sleep and behavior? If the bowel movement problem has had a sudden onset and is quite strong, it can also be important to inquire what the parents have done already and whether they have consulted their doctor. A complete stoppage with sudden onset can be a dangerous condition that requires proper medical investigation and attention. It will, of course, be important to discuss the diet of the child with the parents and make some simple recommendations as needed, to help improve the diet if there appears to be problems with it. This can include discussing whether there may be sensitivity to certain foods such as cow’s milk products. Problems of constipation can occur as a symptom of the spleen or large intestine. If the pattern is spleen vacuity, look also for other signs such as abdominal bloating (independent of the effects of extended episodes of constipation), general abdominal pain, whether the stools have been passed or not, tendency towards also having periods of loose stools or diarrhea and tiredness. If the large intestine, this steers one towards considering the lung vacuity pattern; look for other problems such as nasal congestion, lung congestion, breathing difficulties, skin problems. Occasionally the problem of constipation arises as a sequela of the “kanmushisho”: look for associated problems with behavior or sleep. If there appears to be such problems, the non-pattern-based root treatment may be enough to deal with this, but it could show a problem of the liver channel. In this case examine the child for the liver vacuity pattern, but be careful to check out also whether the liver is not replete as a secondary problem to the underlying lung or spleen vacuity pattern. Since the problem manifests in the digestive system, it is usually enough to use the earth-source points for treatment. These are normally used for the lung (LU-9, SP-3) and spleen (SP-3, PC-7) vacuity patterns, but if the liver vacuity pattern shows LR-3, KI-3 may be better instead of the usual LR-8, KI-10. For the smaller child apply the stroking and tapping or tapping non-pattern-based root treatment as usual over the limbs, back, and abdomen. Apply targeted tapping to the area around GV-12, GV-3 to GV-4, the navel, LI-4, and on the stomach channel below the shins. Tapping at ST-25 and BL-25 can be helpful. Also apply stroking or pressing in a circular motion (following the colon) over the abdomen around the navel (Fig. 20.1). This latter can be ticklish for some children, making it difficult to apply. In such cases use only a pressing technique with a larger instrument such as the round ball end of the enshin. Fig. 20.1 Normal stroking plus extra stroking clockwise around abdomen. Tapping: • Around LI-4 • Around CV-12: five to 10 times • ST-25 area: 10 times each • Around ST-36–ST-37: five to 10 each leg • Sometimes around pubic region: 10 to 20 times • Around GV-20: five to 10 times • Occipital area: 10 to 15 times • Around GV-12: 10 to 20 times • Around GV-3: 10 to 20 times In general, for the treatment of constipation we can focus treatment to the main “constipation” points such as ST-25, BL-25 (Hyodo 1986). Leaving press-spheres at one or both of these points can be helpful. On children who are still in the oral phase and tend to place what they lay their hands on in their mouths, it is probably advisable to avoid leaving the press-spheres on ST-25 as the child may see and get hold of them, and thus potentially swallow them. If on a younger child the press-spheres are not producing a sufficient change one can increase the dose by using press-tack needles. Depending on the child, this is probably better done only to the points on the back (BL-25). For the older child who can handle a larger dose of treatment, one can start by placing press-tack needles on BL-25. If one wants to also stimulate ST-25, apply press-tack needles on BL-25 with press-spheres on ST-25. If there is no change with treatment and one wants to increase the dose again, use of the 3 mm intra-dermal needles to, for example BL-25, can be very helpful. If you choose to use press-tack or intra-dermal needles on the abdomen at ST-25, make sure that the parents are aware of this, and do not do this if you think the child might interfere with them. On the adult we can apply intra-dermal needles or the short press-tack needles (0.6mm) to the “constipation” zone in the ear. This lies along the lower border of the triangular fossa region. On an older child (6–7 years or older) who is not responding to what you have done with enough change, it can be possible to apply the 0.6-mm or 0.3-mm press-tack needles to this region of the ear on one side with appropriate care instructions to the parents. This is not a good idea to try on the younger child because of the risk of their interfering with the needle. On a younger or more frail child, if leaving press-spheres on acupoints such as BL-25 and ST-25 is not producing enough change, one can start applying needling shallowly at acupoints such as ST-25, BL-25, SP-13 (Hyodo 1986). For the older child one can apply needling to these points earlier in the treatment. If the child is older and stays still for you, you can insert the needles to the abdominal points and then begin the pattern-based root treatment. When you finish this root treatment, you can then remove the abdominal needles. We tend not to use these techniques frequently on children for the problem of constipation, but in more stubborn cases it can be advantageous to try cupping lightly over the lower back and around the navel, using light pressure. If the child’s condition is not changing and you notice clear vascular spiders on the lumbar region that are superficial enough to stab, apply the stabbing and squeezing method to these, removing a few drops of blood from each. This last technique can be difficult to apply on very small children as it can be quite uncomfortable on the low back. For really stubborn conditions it can be very helpful to have the parents start applying a simplified form of the core non-pattern-based root treatment regularly at home. The next case is of the sister of the girl in Case 1. One can see that the effects were also quite remarkable. Case 2 Main complaints: Severe problems with constipation since birth. Pediatrician had identified problems with cow’s milk, which was discontinued and replaced by special milk, but without change in symptoms. She had very hard, small stools. She usually did not pass any and the mother had to pull them out manually. She would wake some nights with abdominal pain. She had dry skin and the mother used oils to moisten this. Additional complaints: At 3 months she had had a bad cold; since then she tended to get a stuffy nose, irritated throat (postnasal drip?) with cough. All other systems were unremarkable. Diagnosis: From symptoms and pulse: lung vacuity pattern. Treatment: Tapping was applied with a herabari on the abdomen, chest, back, arms, legs, and especially around GV-12, GV-23, and GV-20. Using a teishin, right LU-9, SP-3 were supplemented, left LR-3 drained. Press-spheres were placed on GV-12, bilateral BL-25, and ST-25. Second visit—2 weeks later The stools had been much better, almost normal over the 2 weeks, but had become slightly harder again in the last 2 days. Treatment: Tapping with a herabari was applied on the abdomen, back, arms, legs, around GV-4 and GV-12. Using a teishin, right LU-9, SP-3 were supplemented, left LR-3 drained. Press-spheres were placed on bilateral ST-25 and BL-25. The mother was taught to do basic tapping at home daily. Third visit—3 weeks later The stools remained better, staying soft for the 3 weeks. Mother and child enjoyed the daily home treatments. Treatment: Using a herabari, tapping was applied on the abdomen, back, arms, legs, chest, GV-12. Using a teishin, right LU-9, SP-3 were supplemented, left LR-3 and BL-58 drained. Press-spheres were placed on bilateral ST-25 and BL-25. Fourth visit—4 weeks later Bowel movements were normal; no constipation, no hard stools. The nose was somewhat less congested and the cough better, but she still had some problems with coughing. Treatment: Using a herabari, tapping was applied to the abdomen, back, arms, legs, chest, GV-12. Using a teishin, right LU-9, SP-3 were supplemented, left LR-3 drained. Press-spheres were placed on GV-12 and bilaterally on the asthma shu point. Light cupping interscapular region. For financial reasons and because of good progress, treatment was stopped. While it is not uncommon for children to come to our clinics with bowel problems like constipation and for the treatments to generally work well, as is evidenced by the first two cases, not all cases of constipation are simply constipation. We have to be alert to complications that require a change in treatment tactic. Case 3 __________________ Main complaints: Gerald had been struggling with constipation for the previous year and a half. He could go through periods of normal bowel movements but at least several times a month he would have difficulty passing stools, leading sometimes to abdominal pain and a lot of emotional distress. He could go up to 5 days without stools, but when not having a period of being constipated he usually had some bowel movement at least every other day. He had no other problems; appetite, sleep, mood were good. He was a full-bodied, energetic child, with no overt signs of weakness, thus I judged he could handle a slightly larger dose of treatment. Press-spheres were applied bilaterally to BL-25. Second visit—1 week later There was nothing to report. Gerald was a bit relaxed on the day of the treatment. His bowel movements were difficult to assess as yet. Treatment: The same pattern of light tapping was applied as on the first visit. Press-spheres were left on bilateral BL-25 and ST-25 (four press-spheres). I taught the mother to repeat the basic light tapping treatment at home daily. Third visit—1 week later Gerald had had slightly more problems with constipation this week, but it was unclear if this was just a normal fluctuation or a worsening of symptoms. I discussed this with the mother and instructed her to apply the home treatment more lightly, with lighter tapping and fewer taps in each area. Treatment: The same treatment as the second session was applied at a very slightly lower dose (lighter tapping with fewer taps in each area. Fourth visit—8 days later The symptoms were similar to those of the previous week; slightly worse than after the first treatment, but not quite as bad as after the second treatment. I decided to try a slightly stronger treatment. Treatment: The same pattern of tapping was applied as on the first visit. Needling was quickly applied to BL-25 bilaterally. Needles were inserted 2–3 mm, moved up and down very slightly and quickly and then removed. Intra-dermal needles were placed on BL-25 with instructions to remove them by the next morning and replace them with press-spheres. Press-spheres were also retained on bilateral ST-25. Fifth visit—12 days later No change in symptoms; his bowel movements remained erratic and problematic Treatment: The same as on the fourth visit. Sixth visit—1 week later Gerald’s bowel movement problems remained unchanged. I was now concerned as it is unusual not to have a clear response of some kind at least after three or so sessions when treating children of this age. I questioned the mother again to see if I had missed or misunderstood anything. Then the problem finally came to the surface. The constipation problems had begun in a period when Gerald was going through the normal growth stage that is associated with the “terrible twos.” In his struggle to create more space for himself and learn more about his boundaries he had found a pattern of behavior that usually would get his mother to give him what he wanted. If he could not easily get what he wanted he would turn angry and threaten his mother “I won’t go to the toilet then,” following which he would hold his stools, thus creating the episodes of constipation. In other words, he did not have a functional bowel problem, he had the “kanmushisho” pattern and the constipation was how it manifested in him. I thus changed my treatment accordingly. Treatment: Light stroking was applied down the arms (three yang channels), legs (stomach and bladder channels), abdomen (stomach channel), and back (bladder channel). Light tapping was applied around GV-12, GV-20, the occipital margin, and LI-4. Press-spheres were applied to GV-12 and GV-3. I instructed the mother to change the home treatment to use the light stroking and tapping of the areas I had worked on. Seventh visit—1 week later Gerald was more relaxed. He had had no problems with bowel movements this week, managing to go every day, at least a little bit. Treatment: The same treatment pattern as on the sixth visit was applied, with the exception that light needling was applied to the area around GB-20 (which felt quite stiff) and LI-4 after the tapping of those points. He had had normal bowel movements every day, with no distress, and his mood had generally improved. He was no longer using the “no toilet” threat with his mother. Treatment: Same as on the last visit. Ninth visit—4 weeks later Gerald was having normal daily or almost daily bowel movements and he was generally in a better mood. Treatment: Same as on the last two visits. I instructed the mother to continue the home treatment for a while longer and come back if there was any recurrence of the constipation problems. This case was interesting. It shows that simply trying to address the manifestations of the symptom is not always the best approach. As long as I did the usual core non-pattern-based treatment with symptomatic focus to constipation and treatment points specific to constipation, there was no real progress. But as soon as I started treating the underlying problem of the kanmushisho, he started changing more and the symptoms started improving. The actual shift in treatment was quite small, but the effects of the small changes were very clear. The following case comes from the practice of my colleague Manuel Rodriguez of Barcelona, Spain. It shows the sometimes very surprising and powerful effects of this simple and gentle treatment method. Manuel saw this baby for treatment before he had learned the Meridian Therapy pattern-based treatment system. He only treated the baby with a simple form of shonishin. The baby would clearly have fitted the category of “spleen weak constitution” type, but did not need the specific root treatment nor the stronger, more aggressive treatments that can be used for this pattern—see Chapter 25 “Weak Constitution.” Case 1 Main complaints: Paul’s mother, a nurse, was one of my students. She contacted me when Paul was about 2–3 months old because he was showing dermatitis linked with digestive problems. After making an appointment she had to cancel the visit on two separate occasions because she had to take Paul to the emergency room at the hospital, where he was subjected to extensive testing. Finally, at the third attempt to schedule an appointment, she brought Paul to my clinic when he was 7 months old. His medical history was already complex. History: November 2002: Paul was born by normal birth after a normal pregnancy. December–January 2003 (while 2–3 months old): He showed dermatitis of the toddler (possibly cradle cap) and a tendency to diarrhea. The analysis by the Western medical doctors concluded that he showed lactose intolerance. They stopped giving him cow’s milk derivatives, giving instead rice “milk” together with cereals. Almost immediately the baby started with major episodes of diarrhea, with frequent passing of semi-liquid feces. The mother started testing different kinds and brands of “milks,” including Damira, a hypoallergenic preparation. Paul continued with the diarrhea, which was becoming increasingly strong. Finally his doctor had him admitted to San Juan de Dios, the most famous pediatric hospital in the area. March 2003 (at age 5½ months): He was still in the hospital. All allergy tests were negative. He was showing hypersensitivity only to egg white (which he had never eaten). Meanwhile the strong symptoms of diarrhea continued. He was referred to the gastroenterology department in the same hospital, where they also were unable to determine the cause of the diarrhea. By this time defecation immediately followed eating anything, and the child was showing deterioration (low weight, failure to thrive). The mother decided to change hospitals and took the baby to another one (Teknon, a private hospital with an outstanding reputation). Once inside this hospital the testing continued. When starch and fat appeared in his stools the pediatrician concluded that Paul had “intolerance to macromolecules” and, after a further round of tests, determined that he had a “deficit of alpha-1-antitrypsin,” which is considered congenital and without any possible treatment. Mid-June 2003: He developed a fever. Within 3 days mucus started appearing in the stools. He was given cefuroxime, an antibiotic. The fever stopped but the diarrhea increased. Early July 2003: He showed signs of dehydration (apathy, loose skin, etc.). He was taken back to the Teknon Clinic where he received emergency treatment. He was discharged 5 days later. The next day, his mother brought Paul to see me for treatment. He looked almost normal, he was only a bit small for his age and his vitality was slightly under par. His skin had a lackluster appearance. He had no dermatitis and there was nothing else to remark on. At this time he was still defecating four or five times a day, always immediately after eating. He had liquid feces with almost undigested food in them. The hospital had informed the parents that they had no treatment to offer. Treatment: I treated him with shonishin, the core non-pattern-based root treatment. To do this I applied very light stroking with a silver enshin over each of the indicated areas (down the arms, down the legs, down the back, down the abdomen). I added a very soft digital massage or pressure over ST-25. I instructed the mother to repeat the light stroking treatment daily at home and to call me in 3 days to let me know how he was doing. Three days later Paul’s mother reported by telephone that starting right after the treatment 3 days earlier, the feces had started to become more consistent. The day after, the child had defecated only three times, with almost normal feces. I instructed her to continue the treatment and report again in 15 days, or to call earlier if something happened. Two weeks later His mother reported by phone that Paul was now defecating only twice a day with normally formed feces. He had been gaining weight and increasing in vitality. I instructed her to continue with the treatment as a way to help the child’s development. At later follow-up (3 and 9 months) the mother reported that Paul’s problem of diarrhea had never returned. He appeared to have a normal digestive system. I discharged him from treatment as he no longer needed any.
Constipation
Hanna, Girl Age 2½ Years
 General Approach for Patients with Constipation
General Approach for Patients with Constipation
 Most Likely Pattern-based Root Diagnosis
Most Likely Pattern-based Root Diagnosis
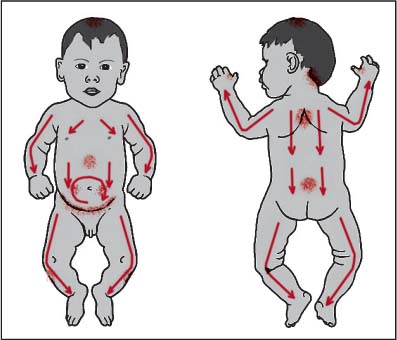
 Typical Non-pattern-based Root Treatment
Typical Non-pattern-based Root Treatment
 Recommendations for Symptomatic Treatment
Recommendations for Symptomatic Treatment
Press-spheres (Ryu), Press-tack Needles (Empishin), and Intra-dermal Needles (Hinaishin)
Needling
Cupping and Bloodletting
 Other Considerations
Other Considerations
 Further Case Histories
Further Case Histories
Alexandra, Girl Age 9 Months
Gerald, Boy Age 3 Years1
Diarrhea
Paul, Boy Age 7 Months
Digestive Problems
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


