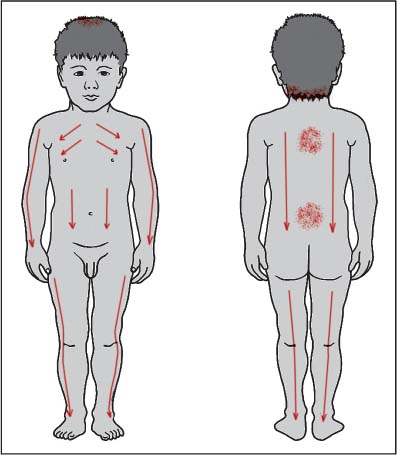
24 Developmental Problems This is a broad category that includes children who, from birth, have had developmental problems such as growth abnormalities (limbs, organs that do not develop properly or at all, spina bifida, etc.), genetic mutations, mental development problems (autism, Down syndrome, mental retardation), complications of intrauterine growth or birthing (such as cerebral palsy). It also includes children who have an accident or disease that leaves them damaged (e.g., mental development problems due to head trauma, loss of locomotor function due to viral infection such as polio). The text by Yoneyama and Mori (1964) discusses the treatment of the sequelae of polio. While we hardly ever see such patients today, we can apply some of the same principles of treatment more generally. Many of the children with the above type of problems usually need special care. Most commonly we see children with these problems who are not institutionalized and live at home with their parents. They are often receiving special medical care or go to special schools that cater to their needs. In some children there is a single problem such as non-use of the legs; in others a broad spectrum of problems affecting multiple developmental and functional systems. In some children the treatment helps create real substantial change and improvements. In others, the treatment helps lessen difficulties, improve function, mood, performance, improve the quality of life for the child, and create a better environment and interaction with their environment. Case 1 Just 3 weeks before going on a summer-long study trip to Japan I received a phone call from a mother in New York, a 1-hour flight away. She had got my name because she was looking for an acupuncturist who treated children and had not been able to find anyone closer. Her daughter Catherine was born with cerebral palsy. At that time she was around 33 months old. Main complaints: She had no use of her legs. If she was laid down she could not push herself into a sitting position. She was unable to walk, even with assistance. Catherine was under care at the local children’s hospital. She was primarily managed by a pediatric neurologist and was seeing a pediatric physical therapist to see what else could be offered. The neurologist had recently indicated that since there was no change in Catherine’s condition, he was projecting that she would probably end up either in a wheelchair or, if lucky, she might be able to walk wearing metal braces as support, but that did not seem so likely. The mother was not happy to hear this, as it indicated that the doctors could not offer much more help for Catherine. Her mother reported that Catherine had no problems with the arms, head, or neck. She had normal control of bladder emptying and bowel movements. Her appetite was good and she was quite a quick-minded, concentrated child. Could I help and how should we proceed? We organized for the mother to bring Catherine up to Boston by plane early the next week to come for a 1-hour appointment where we would start treatment. Once scheduled, I thought about what could realistically be done. In cases such as this, the literature in Japan suggests regular shonishin can be helpful but that one often needs to use okyu/direct moxa on the lower back to help trigger change. I was concerned about the lack of time we had to schedule many treatments, given that I was leaving soon for Japan. Also, while I wanted to have the mother start doing home treatment as soon as possible, I felt I could not apply direct moxa without the ability to be present at follow-up and certainly could not imagine having the parent try home moxa without my supervision. Thus, I planned to do a short core non-pattern-based root treatment, apply minimal light symptomatic treatment, and spend the rest of the hour teaching the mother how to do treatment daily at home. I saw Catherine before I had properly learned Meridian Therapy and thus was unable to add any specific pattern-based root treatment to my treatment for her. The tools available to me were basic shonishin and simple symptomatic methods only. Catherine was a very bright-eyed, strong-willed child (strong in a positive sense, not as a very strong-willed, resistant child). She had little voluntary control over her legs and no strength in them. Thus, for all intents and purposes she was paralyzed from the waist down. Once she was laid on the treatment table she could not raise herself as she did not have sufficiently developed back muscles to allow her to do this. Her sleep and mood were good, appetite and digestion good. She had no other health problems. Treatment: Using the same instruments that I wanted the mother to take home and use daily at home, I gave the following treatment: Using a zanshin-type instrument I applied light stroking down the arms (three yang channels), legs (stomach and bladder channels), back (bladder channel), abdomen (stomach channel and ren mai). Using a herabari, I applied tapping around GV-12, GV-4 to GV-3 area, and then some additional tapping along the spine and around GV-20. Rather than use moxa at the GV-3 to GV-4 area I chose to use a hand-held “electric moxa” instrument. Basically this was a simple device; once plugged in and turned on, a rounded surface with an area about 3 cm in diameter became warm. Holding the instrument with one hand, I could apply a warming heat via this rounded surface to the area over and around GV-3 to GV-4. I did this until the area became slightly pink and warm to the touch. During the treatment Catherine became quite relaxed and seemed very comfortable. I then spent the rest of the hour explaining to the mother how to do the same treatment using the same instruments at home daily. I double-checked her techniques to ensure that she had understood my instructions properly. She agreed to call me in the next 7–10 days to let me know how things were going, and said that she would bring Catherine back for another treatment before I left for Japan if it seemed necessary. Her mother called 10 days later very excited. She had been doing the treatment I taught her daily at home and Catherine really enjoyed it, even expected it. That day Catherine had, for the first time, been able to push herself into a sitting position. I discussed this with the mother and instructed her to continue daily treatment. I would contact her in a few months once I was back from studying in Japan. I called the mother about 20 weeks later to see how things were going and to see if we should schedule further treatments in Boston. The mother was very happy. Catherine was already walking if her hands were held. She was improving rapidly. Because her condition was progressing well I told the mother that she had become the therapist and to continue treatment regularly. She joked that Catherine would not allow her not to do the treatment if she had forgotten or was running behind schedule. I called the mother again about 8 months later to see how things were going. Despite the dire predictions of the pediatric neurologist specialists, Catherine was now walking on her own and could walk up to 30 meters unaided. She was also able to jump a little. She was continuing to make progress with the daily treatments. We discussed how she was progressing and decided that it was unnecessary to come up to Boston to see me. I congratulated the mother for being such a good therapist. When a child faces a lifetime of difficulty due to such circumstances, the ability to trigger changes like this when the doctors are unclear if they can make any real impact is truly moving. It is a lifetime of change that the shonishin treatment created. For a similar case, please also see the case of the child with paralysis and other complications from spina bifida from the caseload of Kazuko Itaya (Manaka, Itaya, and Birch 1995, pp. 307–308). Often the conditions you will be treating are not curable. The goal of treatment is to help lessen the symptomatic manifestations of those problems that are not curable and to increase function for the child. A secondary goal of treatment is to help the parents find additional tools that help with daily functioning and coping for and with the child. The kidney vacuity pattern is the most common. In many cases there will be kidney weak constitution and the recommendations in Chapter 25 “Weak Constitution” can be helpful. Thus, applying supplementation to KI-7 and LU-8 is often useful. Variations of this can include modifying point selection according to symptoms. Thus, if there are any signs of counterflow qi, use of the he- sea points such as KI-10 and LU-5 is indicated. If there are significant problems with strength and use (classical description is “heaviness”) of the limbs, the shu-stream points (KI-3, LU-9) may be useful to try. Additional treatment directed to BL-23 to support the treatment of the weak kidney channel is also indicated. Liver vacuity pattern may also show, but this is more likely in older children. With babies and small children we generally select kidney vacuity pattern as a matter of course since we treat this as a kidney weak constitution problem. But on older children where you are able to obtain pulse and abdominal findings the liver vacuity pattern may appear, especially in children with locomotor disorders and especially associated with spasticity of the muscles. In such cases treating the usual LR-8, KI-10 or LR-3, KI-3 will be most useful according to symptomatic manifestations. For the child with mental development problems, examine the heart pulse carefully. If it seems weak, you can supplement HT-7 or PC-7 as a secondary pattern. Thus, for the kidney vacuity pattern child with mental development problems, after supplementing, for example, KI-7 and LU-8 on one side, supplement HT-7 or PC-7 on the other side of the body. The core non-pattern-based root treatment is helpful with additional tapping targeted at regions according to the symptomatic manifestations. Thus, stroking down the arms, legs, abdomen, and back with tapping around GV-12 is good for most conditions. Additional tapping around GV-12 for upper limb problems will be helpful, as will tapping around GV-3/GV-4 for lower limb problems and on the occipital regions, GV-12 and GV-20 for mental development problems. Sometimes a light pressing around GB-20 and LI-4 can be helpful for children with mental development problems (see Fig. 24.1). Fig. 24.1 Light stroking: • Down the arms (yang channels) • Down the back (bladder channel) • Down the legs (stomach and bladder channels) • Down the abdomen (stomach channel) • Across the chest Light tapping: • GV-20 area: 10 times • Occipital area: 10 times • GV-3 area: 10 times • GV-12 area: 10 times • If problems with the upper limbs: more tapping around • GV-12 (20 times or more) • If problems with the lower limbs: more tapping around GV-3 (20 times or more) For problems of mental development, if the additional tapping or pressing has not been helpful, consider inserting needles lightly to acupoints such as GB-20, LI-4 with an in-out technique. Be careful of the dose and make sure to cause no discomfort with the needling. For problems of the upper limbs, if additional tapping has not been helpful, you can add in-out insertion to acupoints such as LI-4, LI-10, LI-11. If the shoulders or interscapular regions are very stiff and there are knots in those regions, you can apply in-out needling on these knots on older children. For problems of the lower limbs, if additional tapping has not been helpful, you can add in-out insertion to acupoints such as ST-36, GB-34. You may also find knots on the low back/buttock regions, such as lateral to the sides of the sacrum. Needling these knots can also be helpful. Press-spheres or press-tack needles are usually safe to use for musculoskeletal problems, provided the child is not very rundown or overly sensitive. Leaving press-spheres on GV-12 for upper limb problems and around GV-3 to GV-4 for lower limb problems can be helpful. If you leave press-spheres or press-tack needles on other points or areas, make sure to use appropriate dosage levels for the child. Since many children will be kidney vacuity pattern, leaving something on BL-23 bilaterally can be useful, provided you have paid attention to the dose. For children with mental development problems, the dose needs to be much more carefully controlled. If you leave anything, leave only press-spheres to start with. Only use stronger dose techniques like press-tack needles when you are more certain of how the child responds to treatment. The extra point behind shen men on the ear can be treated with press-spheres. If you find a lot of stiffness or knots on the upper back, especially in the inter-scapular region, you can apply treatment to those to help reduce the reactions; it is especially helpful to focus on reactions at BL-15 or BL-14 if they are present. If the problem includes paralysis or problems of use of the upper limbs it is recommended to apply moxa to GV-12 (Irie 1980, Shiroda 1986), GV-13 or GV-14 (Yoneyama and Mori 1964). If the problem includes paralysis or problems of use of the lower limbs apply moxa to GV-4 (Yoneyama and Mori 1964) or GV-3 (Shiroda 1986). In general, for something like cerebral palsy GV-8 can also be treated with moxa (Irie 1980), especially when there are problems of muscle spasticity. Shiroda (1986) mentions use of okyu on GV-12, BL-18, GV-3, and GB-34 for “childhood polio,” which, given the rarity of this today, we can interpret to mean disorders resulting in diminished or lost use of muscles, with difficulty of use of the limbs. If you are thinking of trying the direct moxa treatment, palpate the spine first to see which points are more reactive (exhibit pressure pain, cause the child to flinch or move away) and apply moxa to the more reactive points. In general these techniques are not mentioned much for treatment of this range of problems. If you use either technique be especially careful of dose, and limit its use for children with locomotor problems rather than mental development problems. As is illustrated in Case 1 above, giving the parents tools for home treatment can be very powerful as a way of empowering the parents and speeding up treatment progress. It is more difficult when there are mental development problems to give advice for home treatment. You need to spend more time observing the child’s responses to your treatments to better understand sensitivity and dose requirements. But for other more physical developmental problems, the home treatment can be started as soon as feasible. Again, make sure that you exercise care with the more rundown or very sensitive child. For home treatment, using the simple combination of soft stroking mixed with light tapping is usually a good idea. The next case is of a child with a severe disorder due to genetic mutation with physical, neurological, and mental developmental problems. Case 2 Main complaints and history: Dianne had “Rett syndrome.” She had a complex of problems that included the following: Her parents were told that this condition can be progressive and that she needed regular monitoring and possibly strong interventions in the future.1 She had no history of surgery or hospitalization. She received craniosacral therapy regularly, and her parents were trying a variety of different techniques at home to help with the locomotor problems and mental abnormalities. Although her manifestations were so far quite mild, it was unclear how far the problems might develop. However, she did not appear to be excessively weak. We decided it was worthwhile trying a course of at least eight treatments to see what the treatment did for her. __________________ Examination: She appeared to be quite wary and scared. It was difficult to remove the thumbs from her mouth because of her lack of ease with the new situation. The muscles over the neck, shoulders, back, jaw, and face were very stiff. Left deep pulses stronger than right deep pulses. Abdominal diagnosis was difficult, but indications of a little softness below the navel and depression in the lung reflex area on the right. Diagnosis: Lung vacuity pattern was chosen (based on pulse and other findings). Stomach and/or large intestine channel involvement was suspected because of the jaw tightness and mouthing/biting problems. Treatment: Using a herabari, light tapping was applied over the arms, legs, neck, shoulders, head, and back. Light stroking was applied down the legs and abdomen using an enshin. Supplementation was applied to right LU-9 and SP-3 using a teishin. Stainless-steel press-spheres were applied to GV-12 and bilateral BL-23. Second visit—15 days later At times, the pronation of the right foot was better. She seemed to have greater ease climbing the stairs, and had possibly shown a little more presence with her parents. The press-spheres had caused a minor skin irritation. Treatment: Using a herabari, light tapping was applied over the arms, legs, back, abdomen, neck, shoulders, head, and jaw. Light stroking with an enshin was applied down the back and the neck. Using a teishin, supplementation was applied to right LU-9 and SP-3. Stainless-steel press-spheres were left around GV-13 and bilateral BL-23. Third visit—20 days later She was much more active than usual. She was hand-mouthing a little less, but biting things a little harder (as compensation?). Her hands were warmer. She seemed to be a little more functional and more responsive to parental requests. Treatment: Using a herabari, light tapping was applied over the arms, legs, back, abdomen, neck, shoulders, head, and jaw. Light stroking with an enshin was applied down the arms and legs. Using a teishin, supplementation was applied to right LU-9 and SP-3. Stainless-steel press-spheres were left around bilateral TB-17 and bilateral BL-52. Fourth visit—6 days later There were no clear changes to report. Maybe she was hand-mouthing less, but it was not so clear. Treatment: Using a herabari, light tapping was applied over the arms, legs, back, abdomen, neck, shoulders, head, and jaw. Light stroking with an enshin was applied down the arms, legs, and back. Using a teishin, supplementation was applied to right LU-9 and SP-3. Stainless-steel press-spheres were left around bilateral ST-37 and bilateral BL-23. Fifth visit—2 weeks later She had had a bad flu the week before, but was now recovered. No clear changes in her condition. Treatment: Tapping over arms, legs, abdomen, chest, back, neck, head, and jaw with the herabari. Stroking was applied down the arms, legs, and back with the enshin. Using a teishin, LU-9 and SP-3 were supplemented and left LR-3 was drained. Press-spheres left at bilateral BL-23 and ST-40. Sixth visit—1 week later Treatment was very similar to the last visit. Seventh visit—1 week later Treatment was again similar to the last visit, with the exception of the insertion of 0.12-mm gauge needles shallowly for about 30 seconds to GB-20. After this the parents reported a small reduction in the hand-mouthing and more use of the hands for pointing at things. Eighth visit—1 week later Treatment was similar to the last visit. Ninth visit—2 weeks later The parents reported that her sleep was better, she was walking better, hand-mouthing was better, and that there was more use of her hands. She was more sociable and made more efforts at oral communication. Because of this apparent success, the same treatment as the last was repeated. This produced an immediate adverse reaction. She became very fearful, tired, and unwilling to walk. She needed to sleep a lot after treatment. These symptoms persisted over the next few days. It was obvious that she had been over-treated. Tenth visit—1 week later Her locomotor abilities had regressed this week, while her hand-mouthing remained somewhat improved. A lighter variation of the same treatment was given with light needling at ST-36 instead of GB-20. A week later her walking was still not so good, and the same treatment was repeated. At this time my teacher Toshio Yanagishita was visiting. On consulting him it became clear that a much lighter treatment should be given, eliminating the tapping with the herabari and replacing it with extremely light stroking with the teishin along the stomach and large intestine channels, down the abdomen and back and neck regions. He also advised that her pattern was a kidney pattern and that she should be treated as such. He also commented that in cases like hers the spleen was typically slightly replete, but that this should be treated by supplementing ST-36. Twelfth visit—2 weeks later Treatment: Following the recommendations of Mr. Yanagishita, the treatment consisted of applying very light stroking with the teishin down the large intestine and stomach channels on the arms and legs, twice each channel, down the abdomen twice, down each side of the back twice, and down the neck twice, with a light rubbing with the enshin down the back of each leg. Supplementation was applied to right KI-7, LU-5, and left ST-36. This revised treatment worked better for Dianne, with more consistent improvement and no more adverse reactions due to over-treatment. Over the next 8 months, 22 similar treatments were applied with small variations. Her symptoms overall gradually improved. Occasionally draining techniques were added to points like TB-5, GB-37, BL-58. Press-spheres were left on points like ST-36, GV-12, BL-23. At the end of these 8 months of treatments she went to a special clinic for a full evaluation of her condition. The doctors were very surprised that her scoliosis had not progressed at all (usually it progresses in this syndrome) and that her back seemed to be in quite good shape. Her walking was clearly better. Her hand-mouthing was clearly better; she was also more communicative and participatory. The medical team that evaluated her recommended that the parents apply a daily tactile stimulation on her body by using soft brushes and brushing on the torso and limbs. The parents started doing this at home daily. Fifteen similar treatments were given over the next 6 months. During this time, she became more participatory and started interacting with other children better. Her walking became more stable. However, she showed increasing signs of counterflow qi, with stronger and stronger emotional outbursts, especially angry outbursts, and showed repeated flushing of the face, neck, and shoulders. She became extremely ticklish, and showed increasingly difficult resistant behavior. She would show signs of hyperactivity and signs of extreme fatigue as well. While the home treatments that the parents were doing daily seemed to be helping her physical coordination, it seemed that she was being over-stimulated and had developed counterflow qi reactions as a result. The parents were advised about the possibility that this was happening and that they should cut back on or stop the home brushing. Also, after consulting Mr. Yanagishita again, the side of treatment was changed to the left side and the treatment was made lighter again. At the 50th treatment supplementation was applied to left KI-10 and LU-52 with right ST-36. __________________ Following this change in treatment side, she started becoming less irritable, could sleep better, and showed fewer signs of counterflow qi. As she became calmer she became more communicative again. But the brushing was continued. Five similar treatments were applied over the next 2 months, then she returned to the special clinic for a further evaluation. They were very pleased with her progress but stated that she seemed to be too sensitive to the tactile stimulation and that it should be cut back to only a very small amount each day. Over the next 8 months, 21 treatments were given. During this time her concentration and social skills improved. She tried using words more to communicate. She had been assessed by another team and was found to show skills with numbers and counting. She remained calmer, laughing and playing more. She was less scared by change and was more nimble on her feet. Her parents were very pleased with her progress. It is not possible to cure a child of Rett syndrome, but during the 29 months of treatment her condition did not become progressively worse, which is very unusual for Rett syndrome. Her hand-mouthing and biting of hard objects significantly improved, her locomotor coordination improved, her communication skills were better, as were her socializing skills. She showed signs of understanding more things around her and was better able to follow simple instructions in task performance.
Catherine, Girl Age Almost 3 Years
General Approach for the Treatment of Children with Developmental Problems
Most Likely Pattern-based Root Diagnosis
Typical Non-pattern-based Root Treatment
Recommendations for Symptomatic Treatment
Needling
Press-spheres (Ryu), Press-tack Needles (Empishin), and Intra-dermal Needles (Hinaishin)
Okyu—Direct Moxa
Cupping and Bloodletting
Other Considerations
Home Treatment
Further Case Histories
Dianne, Girl Age Almost 4 Years
 Significant neuromuscular problems; repeated forceful hand-mouthing, and some biting of hard objects, resulting in irritation of skin of the hands around the thumbs; excessive salivation
Significant neuromuscular problems; repeated forceful hand-mouthing, and some biting of hard objects, resulting in irritation of skin of the hands around the thumbs; excessive salivation
 Problems with locomotor coordination; poor gait and instability walking; pronation of feet, especially the right foot, left leg weaker and not as well developed as the right leg; mild scoliosis; some weakness of arms and wrists
Problems with locomotor coordination; poor gait and instability walking; pronation of feet, especially the right foot, left leg weaker and not as well developed as the right leg; mild scoliosis; some weakness of arms and wrists
 Mental abnormalities and autistic tendencies
Mental abnormalities and autistic tendencies
 General problems such as the tendency to have diarrhea and the need to continue wearing diapers because of the inability to self-regulate bowels or urine
General problems such as the tendency to have diarrhea and the need to continue wearing diapers because of the inability to self-regulate bowels or urine
Developmental Problems
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


