Nasal Dermoid
Glioma
Encephalocele
Hemangioma
Teratoma
Diagnosis and Evaluation
Physical Examination
Noncompressible mass between columella and glabella.
Does not transilluminate.
Negative Furstenberg sign.
Broadening of nasal dorsum.
Widening of the anterior nasal septum.
Sinus opening may be difficult to see unless it contains sebaceous material or a hair follicle.
Imaging Evaluation
Preoperative imaging is mandatory in order to assess for intracranial extension as well as the extent of the cyst, with computerized tomography (CT) and magnetic resonance imaging (MRI) giving complimentary information. CT provides information on boney anatomy, whilst MRI determines the soft tissue characteristics. Traditionally, many centers have performed both investigations. However, with a heightened awareness of the potential long-term complications from the radiation exposure in CT, MRI is being increasingly utilized as a solitary investigation [13].
Computerized Tomography
Fine-cut CT (1–3 mm) of the anterior skull base is suggestive of intracranial extension if there is widening of the foramen cecum, a bifid crista galli, or a boney defect in the skull base. However, a fibrous attachment to the dura, without intracranial extension of the cyst may result in a widened foramen cecum and bifid crista galli, therefore mimicking intracranial extension on CT [14].
Images should include the entire nasal, ethmoid, and orbital region from the tip of the nose through the anterior cranial fossa. Contrast should be used in cases of infection and to differentiate a boney defect from enhancing cartilage as well as to differentiate between enhancing nasal mucosa and nonenhancing dermoids.
Magnetic Resonance Imaging
Multiplanar, high-resolution MRI using T1 images, fat-suppressed T2, fast-spin echo inversion recovery pulse sequences as gadolinium-enhanced, fat suppressed T1 images are used to deliver improved soft tissue resolution, particularly in patients who are suspected of having intracranial extension (Fig. 15.1).
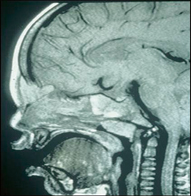
Fig. 15.1
MRI scan in sagittal section demonstrating intracranial extension of a nasal dermoid
Gadolinium contrast helps differentiate dermoids from other enhancing masses such as hemangiomas or teratomas.
Pathology
Macroscopic examination reveals a well-defined cyst lined by squamous epithelium of ectodermal origin with adnexal structures (i.e., hair follicle, sebaceous glands, and sweat glands) of mesodermal origin. These adnexal structures allow differentiation of dermoid cysts from epidermoid cysts . Furthermore, unlike teratomas, nasal dermoids do not contain tissue of endodermal origin (Fig. 15.2).
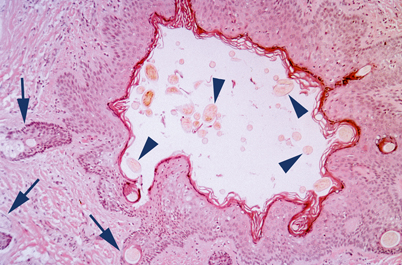
Fig. 15.2
Nasal dermoid characterized by a sinus tract lined by keratinizing squamous mucosa, dermal appendages (arrows), and luminal hair shafts on cross section (arrowheads)
Treatment
Treatment entails complete surgical excision. Conservative procedures such as incision and drainage, aspiration, curettage, and subtotal excision fail to eradicate the cyst, with consequent high rates of recurrence [15, 16].
Surgical Therapy
A wide array of surgical approaches have been described. The optimum approach for each individual patient is determined by the site of the cyst, the site of any tract opening, the presence or absence of intracranial extension, and the surgeon’s experience.
Excision is performed under general anesthesia with a thorough examination of the nasal skin performed under magnification (prior to injection of local anesthesia), as a sinus tract opening may be visible that may not have been appreciated in the office.
In the absence of intracranial extension, the external rhinoplasty approach, a vertical incision over the cyst, a horizontal incision over the cyst, facial degloving approach, endoscopic transnasal approach, and a medial canthal incision have all been described [10].
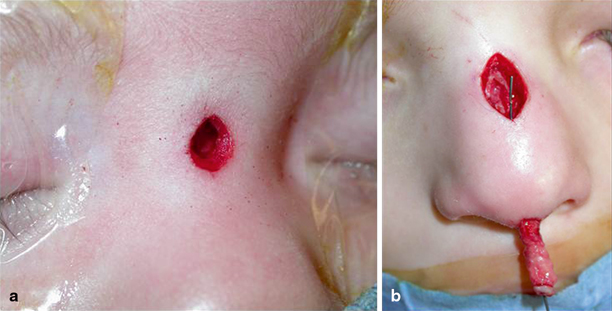
Excision of any sinus tract opening necessitates an incision on the nasal dorsum. Excision of the underlying cyst and tract via a vertical extension of this has remained the most traditional approach. The sinus tract opening is excised using a small elliptical incision and attempts are made to confine the vertical incision to the skin overlying the cartilaginous nose, as it is the senior author’s experience that skin in this area heals more satisfactorily than the skin overlying the boney nasal skeleton. Depending on the location of the cyst, this incision may be in continuity or separate from the elliptical incision around the sinus tract opening. This approach has been suggested to have superior cosmetic outcomes to lateral rhinotomy and horizontal incisions [17, 18] (Fig. 15.3).