34 Dentition and Common Oral Lesions
Dentition
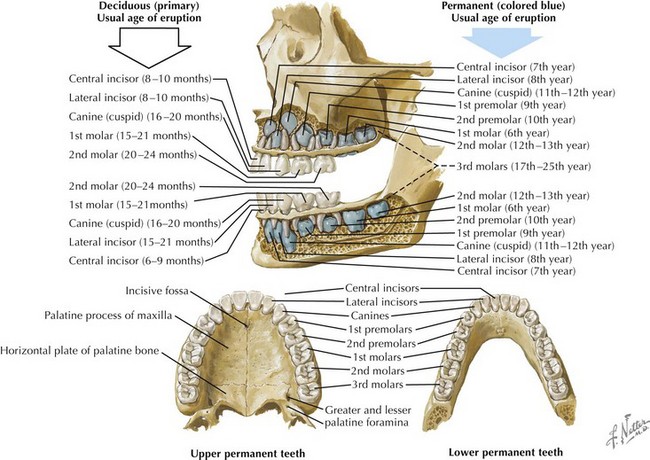
The development of the teeth begins in utero and continues well into adolescence. The 20 primary teeth (also known as deciduous or milk teeth) typically erupt between the ages of 6 months and 2 years. The exfoliation of the primary dentition and the eruption of the 32 permanent teeth usually begin at around age 6 years. On each side of the mouth, the mature permanent dentition consists of maxillary and mandibular central incisors, lateral incisors, canines, two premolars, and three molars (Figure 34-1).
Normal Tooth Anatomy
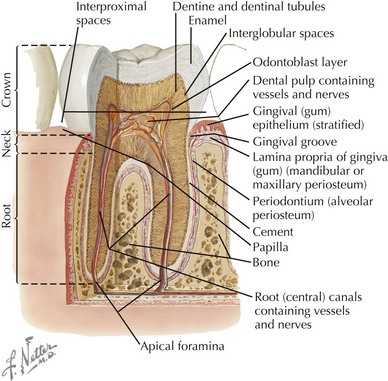
The visible portion of the tooth, which protrudes from the gingiva, is the crown, and its hard surface is an enamel made of hydroxyapatite crystals. The portion of the tooth that connects to the maxillary and mandibular alveolar bones is the root, and its hard covering is called cement. The neck of the tooth is the portion that connects the crown and the root. The periodontal ligament, or periodontal membrane, holds the root in place by attaching the cement to the periosteum of the alveolar bone. Beneath the protective overlying enamel and cement, a layer known as dentin provides the bulk of the body of the tooth. The innermost portion of the tooth, surrounded and protected by dentin, is the pulp chamber, which contains nerves, blood vessels, and connective tissue (Figure 34-2).
Dental Infections
Caries
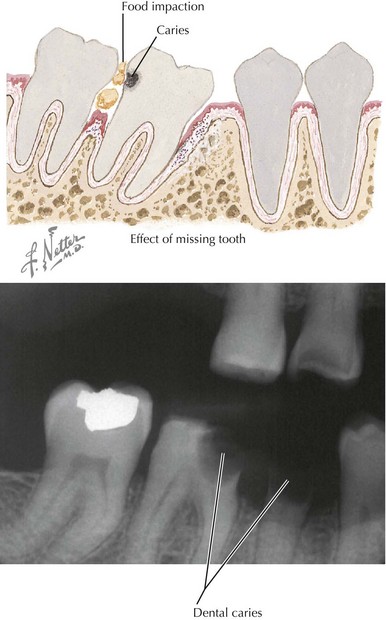
Bacteria, especially the Streptococcus mutans group, are typically transmitted from mother to infant soon after the eruption of the primary teeth. These bacteria colonize tooth surfaces and form plaques above and below the gingival margin. Caries result when these bacteria ferment sucrose from ingested dietary carbohydrate, producing organic acids on the tooth surface. These acids lead to the destruction of the hydroxyapatite crystals that give the enamel its structure, making the enamel more and more porous and eventually causing breakdown of the tooth surface (Figure 34-3). These areas of breakdown can erode through the enamel and dentin into the pulp, where an inflammatory response raises the pressure in the pulp chamber and can cause compression, and thus ischemia, of the pulp vessels. This is known as pulp necrosis.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


