Chapter 20 Congenital Anomalies and Benign Conditions of the Ovaries and Fallopian Tubes
 Congenital Anomalies of the Ovaries and Fallopian Tubes
Congenital Anomalies of the Ovaries and Fallopian Tubes Benign Conditions of the Ovaries
Benign Conditions of the Ovaries
FUNCTIONAL AND BENIGN OVARIAN TUMORS
The human ovary has a striking propensity to develop a wide variety of tumors, most of which are benign. As indicated in Table 20-1, ovarian masses may be functional, inflammatory, metaplastic, or neoplastic. During the childbearing years, 70% of noninflammatory benign ovarian tumors are functional. The remainder are either neoplasms (20%) or endometriomas (10%). The management of ovarian tumors, whether functional, benign, or malignant, involves difficult decisions that may affect a woman’s hormonal status or her future fertility. Although only functional cysts and benign ovarian neoplasms are considered in detail in this chapter, diagnostic methods to differentiate benign masses from malignant ones are discussed.
TABLE 20-1 DIFFERENTIAL DIAGNOSIS OF OVARIAN MASSES
| Pathogenesis | Specific Type |
|---|---|
| Functional | Follicular cysts |
| Lutein cysts | |
| Polycystic ovaries | |
| Inflammatory | Salpingo-oophoritis |
| Pyogenic oophoritis—puerperal, abortal, or related to an intrauterine device | |
| Granulomatous oophoritis | |
| Metaplastic | Endometriomas |
| Neoplastic | Premenarchal years—10% are malignant |
| Menstruating years—15% are malignant | |
| Postmenopausal years—50% are malignant |
Functional Ovarian Cysts and Tumors
A luteoma of pregnancy is a related condition in which there is a hyperplasic reaction of ovarian theca cells, presumably from prolonged hCG stimulation during pregnancy. The luteomas characteristically appear as brown to reddish-brown nodules that may be cystic or solid. A luteoma of pregnancy (Figure 20-1) may be associated with multifetal pregnancies or hydramnios. They can cause maternal virilization in 30% of women and, less often, ambiguous genitalia in a female fetus. Although ovarian enlargement may be impressive, surgical resection is not indicated because luteomas regress spontaneously postpartum.

FIGURE 20-1 Gross appearance of a luteoma of pregnancy. Note the multiple brown nodules.
(From Voet RL: Color Atlas of Obstetric and Gynecologic Pathology. St. Louis, Mosby, 1997.)
Polycystic ovary syndrome, a functional disorder generally associated with chronic anovulation and hyperandrogenism, can also produce enlarged ovaries with multiple simple follicles (Figure 20-2). The hormonal aspects of this syndrome are discussed further in Chapter 32.
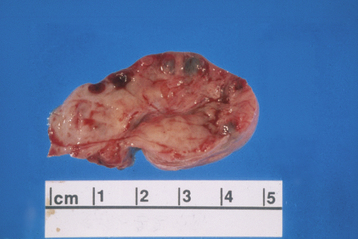
FIGURE 20-2 Ovary with multiple cysts lining the capsule consistent with polycystic ovary syndrome.
(Courtesy of Dr. Sathima Natarajan, Ronald Reagan–UCLA Medical Center.)
DIAGNOSIS
All suspicious adnexal masses in premenopausal and postmenopausal women must be carefully evaluated. Table 20-2 contains a useful risk assessment tool, the risk for malignancy index (RMI), which can be used to help identify those ovarian masses that could be malignant. The RMI has high sensitivity (87%) and specificity (97%).
TABLE 20-2 CALCULATION OF THE RISK OF MALIGNANCY INDEX∗ FOR AN OVARIAN MASS
| Criteria | Scoring System |
|---|---|
| A. MENOPAUSAL STATUS | |
| Premenopausal | 1 |
| Postmenopausal | 3 |
| B. ULTRASONIC FEATURES | |
| C. SERUM CA-125 TITER | Absolute value |
∗ Risk of Malignancy Index = A × B × C. A cut-off value of 200 discriminates a benign from a malignant mass with a sensitivity of 87% and a specificity of 97%.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


