Fig. 11.1
XR and MRI of a 10 y-o male who complains of knee pain. Bone alteration is seen on the XR. MRI shows no affectation of the physis. So limb salvage is the indication in this cases
Suspecting a bone tumor, an MRI scan was taken. Subsequently, the boy underwent open biopsy (of 6 cm of length) with curettage. After this procedure the patient was not able to walk with that leg due to the pain. The tumor was diagnosed as osteosarcoma.
At this point, the boy was brought to our center to receive treatment. After evaluation of the case (Fig. 11.2), we decided that limb salvage was possible by means of the Cañadell technique and posterior reconstruction. The patient started chemotherapy and received three sessions of intra-arterial chemotherapy. We placed the external fixator and distraction was carried out at a rate of 1 mm per day.
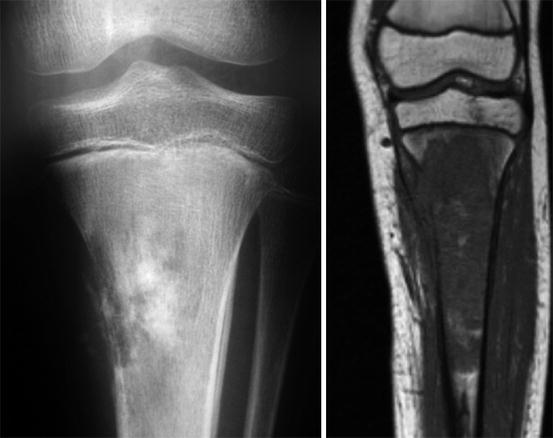
Fig. 11.2
XR and MRI after open biopsy elsewhere. The tumor has grown without the treatment
After between 7 and 10 days of distraction or if the patient reports pain, we typically request an X-ray to confirm rupture through the growth plate. In this case, the X-ray revealed that separation had occurred through the biopsy tract (Fig. 11.3).

Fig. 11.3
Control XR of the external Fixator. We observed that the distraction has not been done through the physis, is been done through the biopsy tract. At this point we remove the EF
The external fixation was removed and intra-epiphyseal osteotomy undertaken. We were able to preserve the proximal tibiae epiphysis and the knee joint. We reconstructed with an intercalary allograft with an intramedullary nail (Fig. 11.4 and 11.5).

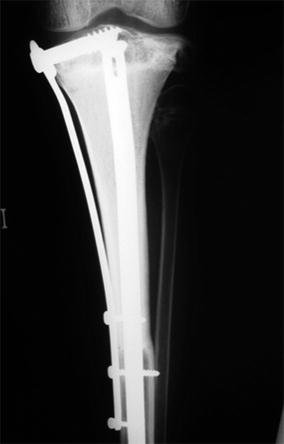
Fig. 11.4
Specimen. We performed an intra-epiphyseal osteotomy. See how we get a secure margin above the physis. Histology showed complete necrosis of the tumor
Fig. 11.5
Postoperative RX of the reconstruction with allograft and intramedullary nail and scaffolding with a plate fixing the rest of the epyphisis. We conserve the articular surface
Postoperatively, the patient recovered in a normal way. He continued with chemotherapy treatment. The excised tumor had 100 % necrosis. The patient started walking with crutches and then with full weight-bearing and demonstrated complete range of motion of the knee.
Nine months after completion of chemotherapy (one and a half years after surgery) the patient reported a pain in the contralateral knee (Fig. 11.6). This turned out to be a single bone metastasis without lung affectation. We decided to treat the metastasis as if it were a primary tumor. Intra-venous and intra-arterial chemotherapy was initiated. As the tumor was in contact with all of the physis, we performed intra-epiphyseal osteotomy rather than the Cañadell technique. Then we proceeded with reconstruction (Fig. 11.7)
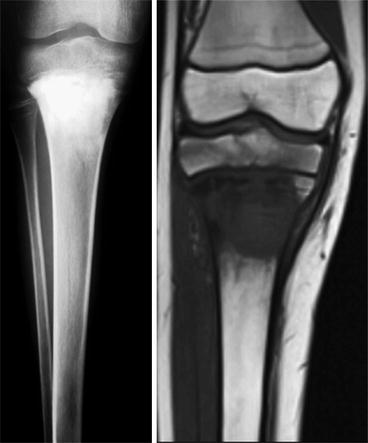

Fig. 11.6
Xr and MRI of the right tibiae. The patient presented a bone metastasis in contact with the whole physis without lung mets. We decided to do an intra-epiphyseal osteotomy as he has before in the other leg
Fig. 11.7




XR control of both legs
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
