Chapter 14 Complications of Gynaecological Surgery
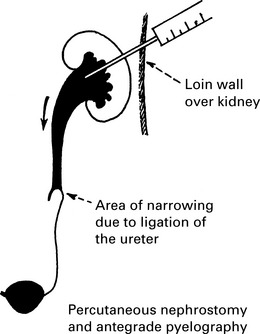
Management of ureteric injury
1. Types of ureteric injury identified at operation.
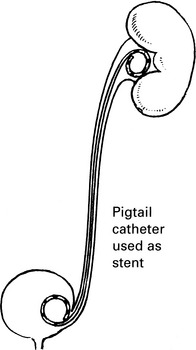
a. Crush injury from clamp or ligature. The clamp or ligature should be removed, and a ureteric stent inserted.
Chapter 14 Complications of Gynaecological Surgery