CHAPTER 24 Choledochal Cysts
Step 1: Surgical Anatomy
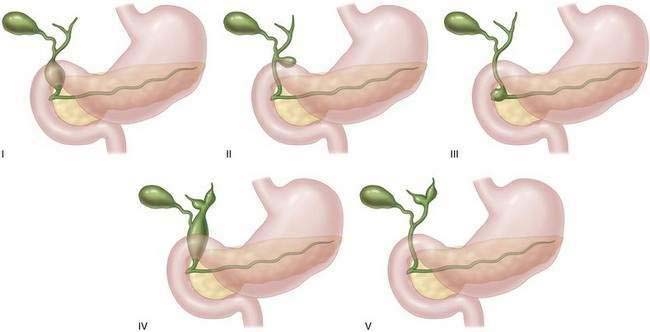
♦ The anatomic configurations of a CdC were first classified by Alonso-Lej and colleagues and subsequently modified by Todani and colleagues into five subtypes (Fig. 24-1).
 Types II, III, and V choledochal cysts are rare variants.
Types II, III, and V choledochal cysts are rare variants.
 Types II, III, and V choledochal cysts are rare variants.
Types II, III, and V choledochal cysts are rare variants.• A type II CdC is a diverticulum arising from the wall of the bile duct. This abnormality is thought to occur because of a localized weakness in a segment of the common bile duct.
• A type III CdC, also known as a choledochocele, consists of a dilatation at the distal end of the common bile duct that protrudes into the lumen of the duodenum. Endoscopically, its appearance is similar to that of a ureterocele found within the bladder.
Step 2: Preoperative Considerations
Presentation
♦ Classically a patient presents with abdominal pain, jaundice, and a right upper quadrant mass; however, rarely are all three present at diagnosis.
♦ Some patients are diagnosed with cholangitis when they present with Charcot triad: jaundice, fever, and right upper quadrant pain.
♦ Others have recurrent episodes of pancreatitis as a result of sludge within a CdC, which causes intermittent obstruction of the pancreatic duct.
♦ A giant CdC can spontaneously perforate. Because bile causes chemical peritonitis, these patients require urgent care.


Diagnosis
♦ Laboratory studies performed in patients with a CdC are often normal. Serum conjugated and unconjugated bilirubin and hepatocellular transaminase levels are within normal limits unless the patient has cholangitis or has developed cirrhosis. In patients who present with pancreatitis, serum amylase levels may be elevated.
♦ Cross-sectional imaging of the abdomen is necessary to define the anatomic configuration of a choledochal cyst. Computerized tomography or magnetic resonance imaging should be used to define the anatomic extent of disease. Hepatobiliary scintigraphy (HIDA) scan is helpful to determine patency of the biliary tract. On occasion, endoscopic retrograde cholangiopancreatography (ERCP) or, more recently, magnetic resonance cholangiopancreatography may be helpful to define anatomy more clearly, especially in cases in which the cyst size is small.
Treatment Strategy
♦ Treatment of a CdC is essential because it will cause recurrent episodes of cholangitis and may cause the development of biliary cirrhosis or evolve into a cholangiocarcinoma. All of these patients will require surgical intervention, but the type of procedure performed varies according to the subtype of CdC diagnosed. For a patient who presents with cholangitis or acute pancreatitis, surgical intervention is delayed until the inflammatory process has resolved.
Step 3: Operative Steps
Types I and IV Choledochal Cyst
♦ A right subcostal incision is used to enter the peritoneal cavity. If necessary, the incision is extended across the midline.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


