CHAPTER 10
Child Advocacy
Marni E. Shear, DO, FAAP, and Grant P. Christman, MD, FAAP
CASE STUDY
A 7-year-old boy is brought to the emergency department by his mother with acute onset of respiratory distress. He awoke from sleep with a coughing fit and has not been able to catch his breath since. His mother explains that her son was admitted to the hospital with similar symptoms 1 month previously and was diagnosed with asthma at that time. Although the boy was prescribed 2 inhalers during his hospital admission, his mother reports she no longer has these because her son has not needed them. She also explains that her child has a daily nighttime cough and frequent coughing with exercise. After administration of an oral steroid load and 3 doses of ipratropium bromide and albuterol sulfate, the child’s breathing improves somewhat. He is admitted to the inpatient pediatric service for ongoing asthma management and care.
Questions
1. What does it mean to be a child advocate?
2. Aside from caring for individual patients, how can pediatricians promote the well-being of their communities?
3. What is the role of the pediatrician in child advocacy?
4. What are the levels of advocacy?
5. How does the pediatrician implement advocacy?
An advocate is someone who speaks on behalf of a person or cause. No group in our society has a greater need for advocates than children. Children are ill-equipped to face the many threats to their health; they cannot obtain their own health insurance, access available social services, or get themselves to the doctor when sick. Additionally, children have limited influence compared with adults in our society. They cannot vote, donate money to political campaigns, or speak publicly to advance their interests. The word “advocate” is derived from a Latin root meaning “one who has been called to another’s aid.” From the beginnings of pediatrics as an independent branch of medicine, pediatricians have answered this call to advocate for the health and well-being of children.
Abraham Jacobi, MD, who is often referred to as the father of pediatrics in the United States, spent his career in the late 1800s and early 1900s advocating for children through legislation in New York and the District of Columbia. He addressed issues such as breastfeeding, food and water contamination, and conditions in foundling homes. He urged physicians to be involved in public life and policy making, and he was the founder and first president of the American Medical Association (AMA) Section on Diseases of Children. Another founder of pediatrics in the United States, Job Lewis Smith, MD, recognized the need for a clean water supply and decent housing to decrease the high infant mortality rate of his time. He worked through public advocacy to improve living conditions for all children, and he was the founder of the American Pediatric Society, which was the first pediatric medical society.
In 1921, the US Congress passed the Sheppard-Towner Act, the first major federal program to specifically address maternal and child health. It provided matching funds to states for services for pregnant women and new mothers. The AMA, which was concerned about government interference in the practice of medicine, condemned the act, whereas the AMA’s own Section on Diseases of Children supported it. Conflict related to the Sheppard-Towner Act ultimately resulted in the pediatric group leaving the AMA and founding the American Academy of Pediatrics in 1930. The American Academy of Pediatrics has been advocating for children ever since.
The New Morbidity
Advocacy remains important because the “new” morbidities in pediatric medicine, some of which are new and others of which are only newly recognized, are related to social and economic forces. Child health outcomes improved dramatically in the 1900s with the development of vaccines, antibiotics, and new and improved surgical care to manage the classic morbidities of infectious disease, infant mortality, poor nutrition, epidemics, overcrowding, and chronic disease. New morbidities that were recognized in the 1960s to 1980s, as described by Robert Haggerty, MD, included family dysfunction, learning disabilities, emotional disorders, and educational problems. In the 1980s to early 2000s, Judith Palfrey, MD, documented new challenges for pediatricians: social disarray, political ennui, the sequelae of high-tech care, and new epidemics of violence, AIDS, cocaine, and homelessness. The newest morbidities of the 21st century include the increased prevalence of childhood obesity, bullying, significant health disparities among cultural and socioeconomic groups, and the growing population of children with special health care needs. Mounting evidence, such as provided by the Adverse Childhood Experiences Study conducted from 1995 through 1997 by the Centers for Disease Control and Prevention and Kaiser Permanente, has demonstrated the critical need to identify and mitigate sources of toxic stress, which can pose a long-term threat to the developing brain.
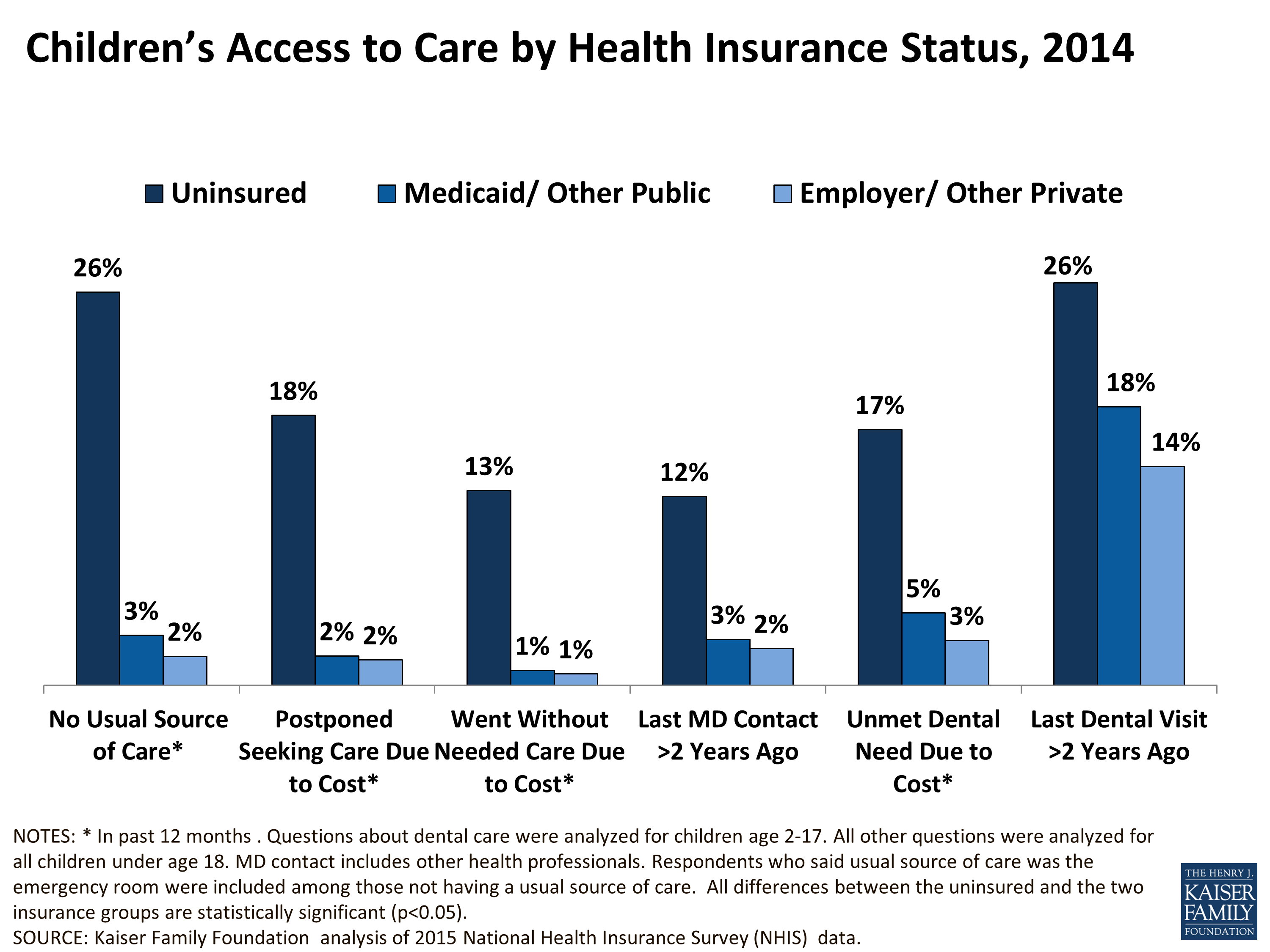
Although improvement has occurred in recent years, many children in the United States continue to face challenges in obtaining access to quality health care. The 2015 National Health Interview Survey found that children without health insurance were less likely to have a usual source of care and were more likely to postpone seeking care than children with health insurance (Figure 10.1). In the past several decades, government programs such as Medicaid and the Children’s Health Insurance Program have expanded the availability of health care coverage to children of limited financial means. The passage of the Patient Protection and Affordable Care Act in 2010 (PPACA) resulted in significant increases in access to health care for many pediatric populations. The number of children younger than 18 years with no health insurance coverage decreased from 6.6 million in 2012 to 3.9 million in 2016; however, 1 in every 20 children remained uninsured as of 2016. Among children in poverty, the uninsured rate was 7%, compared with a rate of 5% for children not in poverty. Racial and ethnic minorities were also more likely to be uninsured, with Hispanic children having the highest rate at 7.9%. As of 2016, approximately 40% of all children were receiving coverage from public insurance programs, an increase from 2010. With ongoing legislative efforts to either repeal PPACA or reduce benefits, the future of access to health care for children remains in jeopardy.
These significant issues affecting child health cannot be adequately addressed on an individual basis. Advocacy on a community or national scale is required to improve child health outcomes and quality of life for children.

Figure 10.1. Children’s access to care by health insurance status in the United States in 2014.
* In past 12 months. Questions about dental care were analyzed for children age 2–17 years. All other questions were analyzed for all children younger than age 18 years. MD contact includes other health professionals. Respondents who said usual source of care was the emergency department were included among those not having a usual source of care. All differences between the uninsured and the 2 insurance groups are statistically significant (P < 0.05). Adapted with permission from Kaiser Family Foundation analysis of 2015 National Health Insurance Survey (NHIS) data. https://www.kff.org/wp-content/uploads/2015/11/children_s-access-to-care-by-health-insurance-status.png
Levels of Advocacy
Every pediatrician serves as a child advocate on a daily basis. With every patient encounter, the pediatrician advocates for care in the best interest of the patient. This first level of advocacy includes treating the individual’s immediate medical needs, that is, performing screening tests, providing anticipatory guidance, and coordinating referrals as necessary. In addition to providing direct medical care, the pediatrician may advance the welfare of the child by, for example, writing letters to help a patient obtain social services, or visiting a patient’s school for a meeting on creating or reviewing an Individualized Education Program.
The second level of advocacy is community advocacy. The AAP policy statement “The Pediatrician’s Role in Community Pediatrics,” describes “community pediatrics” as a perspective that broadens the perspective from a focus on the individual patient to all the children in the community; a recognition that family, education, society, culture, spirituality, economy, environment, and politics all affect the health of children; a synthesis of clinical practice and public health principles directed to providing health care to a child and promoting the health of all children; a commitment to collaborate with the community to optimize health care for all children, especially disadvantaged children; and recognition that community pediatrics is integral to the role of the pediatrician. The pediatrician has a responsibility to improve conditions in the community to benefit patient health. To do this, they must be familiar with the services that are available for children. They can develop relationships with child care centers, schools, community coalitions, city governments, and local organizations to advocate for the best interests of children. Examples of potential involvement in the community include serving as a board member of a community organization, developing health agendas, working with an existing organization to design and fund a community service project, and being a source of information for the community on child health issues.
On the state level (the third level), pediatricians can work to improve health care resources or develop policies to help and protect children. Opportunities for involvement include working on legislation, budgets, regulations, and initiatives or working with the executive branch of local and state government. The fourth level of advocacy is the federal level; at this level, pediatricians can educate their senators and congresspersons on child health issues. Pediatricians may also testify before a congressional subcommittee. The fifth and final level of advocacy is the international level. For example, a pediatrician may choose to work with the World Health Organization to improve immunizations for all children worldwide. Global child health is currently a focus of many advocacy training programs.
At the local, state, and national levels, voting remains a powerful tool for the pediatrician to advocate for child health and welfare. In addition to voting themselves, pediatricians can encourage their patients to register to vote when they reach the age of eligibility.
Becoming a Child Advocate
To become an effective child advocate, the pediatrician must first identify an issue that he or she wants to change or set a goal to improve the lives of children. The more specific the issue or goal, the easier it is to develop a solution. Ideas often arise from clinical practice, in which repeatedly engaging in individual advocacy efforts on behalf of patients with the same problems suggests the need for a larger solution. The first step in taking action is to obtain background information about the problem and collect objective data that support the need for change, then define the nature of the problem and the affected population in clear and precise terms. Child health data from public agencies and private organizations are increasingly accessible via the internet.
Community Projects
Alternatively, a pediatrician may find that an issue is best addressed through a community advocacy project. In developing such a project, the pediatrician’s relationship with the community is of utmost importance, and the pediatrician should endeavor to become familiar with the community as a whole. Community exploration, which may be as simple as walking or driving through a community and observing, can reveal areas of need, such as dilapidated housing or unsafe streets. Equally important is the discovery of the community’s assets, including institutions such as places of worship, schools, and banks, which strengthen a community and are potential sources of support for and counsel about the project. Pediatricians should view themselves as members of the community, acting from within and in collaboration with the community, rather than as outsiders bringing about change externally.
The next step is to develop an intervention. After the possible solutions are considered, the pediatrician should collaborate with community stakeholders to develop and implement the most practical solution. Having credibility in the community makes the task of collaboration much easier. Collaboration requires the ability to compromise and be flexible in developing and implementing plans. Larger projects may require funding, and grants may be sought from advocacy organizations, foundations, the government, or even local businesses. Data should be collected during the intervention to monitor the success of the project and then shared publicly with members of the community as well as with leaders who can shape policy (eg, legislators). If the project is successful, its methods may be adopted by child advocates in other communities.
Legislative Advocacy
Although involvement in the legislative process is initially daunting for the physician without political expertise, often it is the only means by which to effect a desired change for children’s health. Information about the content and progress of existing bills is readily available online, and legislators can be contacted by letter, email, or telephone to offer a position. It is helpful to become familiar with the process by which a bill becomes a law, both at the state and the federal level; the identities of the important players change as a bill progresses through the various subcommittees and committees and ultimately proceeds to a floor vote.
Pediatricians may also arrange to meet with a legislator or staff member at a district or capital office to discuss their position personally. In the dual role of scientist and healer, the pediatrician is in a unique position to inspire both the heart and the mind. It is important to state the problem clearly and explain why a new law is the solution, present well-researched facts that support the position, and use clear language, avoiding medical jargon whenever possible. The pediatrician should minimize the appearance of self-interest by focusing on how the proposal will help children, rather than how it will benefit the profession. It may also help to connect with the legislator by sharing a story about a patient encountered in practice who has been affected by the problem, especially if the patient is a constituent of the legislator (although the patient’s identity must never be discussed without the patient’s consent). Providing the legislator a concise fact sheet summarizing the position and the pertinent background information helps ensure that the position is not forgotten when the legislator is considering the issue at a later date.
The pediatrician should be prepared to encounter opposition from some legislators and avoid responding with angry statements that would be alienating. Effective advocacy requires building relationships with legislators over the long-term, and a legislator who opposes a position 1 year may be a potential supporter the next year, when the political climate changes, or may be a potential ally on another important issue. Among the several other pitfalls to be avoided include making or agreeing with partisan statements or claiming to represent an organization (eg, AAP) or an institution (eg, a university) without authorization. When asked a question to which they pediatrician does not know the answer, it is best to avoid guessing and to instead offer to do further research and provide the requested information to the legislator at a later date.
When developing a new legislative proposal from scratch, it is necessary to remember that although the factors contributing to child health are numerous and complex, each legislative proposal must by nature be concrete and limited. It may be best to start small and work for incremental change. The first step is to identify a clear and, if possible, measurable, objective and define the target population. Other important information to know when drafting a proposal includes any potential funding sources (if applicable) and which government agencies might be involved in implementation or enforcement. The pediatrician should partner with 1 or more legislators early on, not only because a bill must be sponsored by a legislator to be considered for passage but because many of the finer points of the legislative process are outside the experience of the average pediatrician. Building a coalition of support within the community and involving important stakeholders such as politicians, business professionals, other health professionals, educators, and parents, will help the bill gain political support.
Opposition should be expected, and potential sources of opposition should be identified in advance. If opposition from a powerful interest group is anticipated, it may help to meet with a representative of that group to explain the proposal. Potential arguments might include ways in which the proposal is really in the group’s best interest, the moral imperative to help children, or the potential for negative publicity by opposing an initiative to benefit children. Compromising on aspects of the proposal should be considered when doing so might turn a detractor into an ally. When facing intractable opposition from powerful interests, pediatricians and supporters should strive to recruit even stronger allies into their coalition.
The process of turning a policy idea into legislation may be lengthy. It may be necessary to reintroduce a bill repeatedly over several years before achieving passage. After a bill becomes a law, advocates must continue working to ensure that necessary funds are allocated during the budgeting process, that public agencies implement the law as intended, and that the law is reauthorized when necessary. Physicians who are recognized as experts in child health policy will be called on to testify before committees in Congress or the state legislature on policy issues affecting children.
Media Advocacy
The media, including newspapers, magazines, radio, television, and the internet, are extremely influential. News stories about child health and welfare may not always be written from a child-friendly point of view. The pediatrician plays an important role in providing the media with better information and a different angle on a story. For instance, a pediatrician reading a newspaper story about a child who exhibited signs of autism shortly after his 1-year-old physical examination might write a letter to the editor discussing the lack of scientific evidence for a connection between vaccinations and autism. Over time, a pediatrician can develop relationships with local journalists, who can then turn to the pediatrician for information when covering child health stories.
A directed media campaign may also be a key element in an advocacy project. At the community level, the media can help educate the public about child health practices, notify the public of events, and bring out potential allies and coalition members. When advocating for legislation, the pediatrician can use the media to reach legislators directly and, equally important, reach thousands of the legislators’ constituents simultaneously, who may in turn help pressure their legislators for change. In such situations, it is essential to plan a media strategy in advance by determining the most important target audience, selecting the appropriate types of media to approach, crafting a message appropriate to those media, and preparing thoughtfully for encounters with journalists.
Getting Connected
The AAP is a vital resource for pediatricians interested in child advocacy, with opportunities for involvement offered through the AAP Department of Federal Affairs, as well as the various state chapters advocating at the state and local levels. The AAP has also established a network of pediatricians who advocate through social media, using Twitter as a communication platform on which Tweetiatricians can initiate and facilitate conversations on various topics related to child health. A social media toolkit is available through the AAP to help pediatricians choose the best platform for their specific outreach goals. In an effort to promote understanding of the effect of poverty and social determinants on child health, the Academic Pediatric Association has developed a robust curriculum to help deepen understanding of income disparities, social determinants of health, health care delivery systems in the United States, and opportunities for legislative advocacy. Other national organizations with which pediatricians may become involved and that provide advocacy toolkits include Docs For Tots (http://docsfortots.org), Children’s Defense Fund (www.childrensdefense.org), Children Now (www.childrennow.org), the National Center for Children in Poverty (www.nccp.org), and the Child Welfare League of America (www.cwla.org).
Improving the health of all children through advocacy is considered to be the responsibility of pediatricians and can be a tremendously rewarding part of pediatric practice.
CASE RESOLUTION
Managing this child’s asthma is only the first aspect of thorough pediatric care. For the pediatrician to advocate for this patient and prevent a third admission for a subsequent and potentially worse asthma exacerbation, it is necessary to obtain essential information, such as the patient’s social history and the environment in which he lives. A thorough social history is obtained and reveals that the child lives with his mother and grandmother. The mother recently lost her job, and she and her son moved into a 1-bedroom apartment with the child’s grandmother. The apartment has old carpeting, and the mother expresses concern about mold on the walls. The child’s grandmother smokes cigarettes, but she avoids smoking in the apartment when the child is home. The patient and his family are counseled about his diagnosis of asthma and potential asthma triggers. The grandmother expresses interest in smoking cessation, and resources are provided. The family receives an asthma action plan and education on the use of a metered dose inhaler with a spacer, and the pediatrician uses the teach-back method to ensure understanding of the plan of care at discharge. The pediatrician becomes concerned about the high prevalence of asthma in the community and explores coalitions in the area that recognize similar concerns. He becomes a member of the coalition steering committee and works with the local health department and other community stakeholders to develop a home-based intervention program in which community health workers provide families with in-home environmental assessments, education, and support. As a result of the coalition’s efforts, the child’s home is 1 of many apartment complexes in the area assessed by the local housing authority, and resultant action is taken to bring the property up to health and safety standards.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



{kind=link}