10 CEREBROSPINAL FLUID EVALUATION
General Discussion
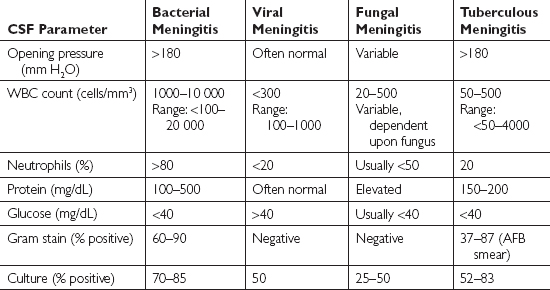
The central nervous system (CNS) is susceptible to bacterial, viral, and fungal infections, as well as to prion diseases and numerous local and systemic diseases. Examination of the cerebrospinal fluid (CSF) is crucial in helping to diagnose infections and other diseases. Although not definitive, certain CSF findings are suggestive of bacterial, viral, fungal, or tuberculous meningitis. These findings are outlined in Table 10.1 below.
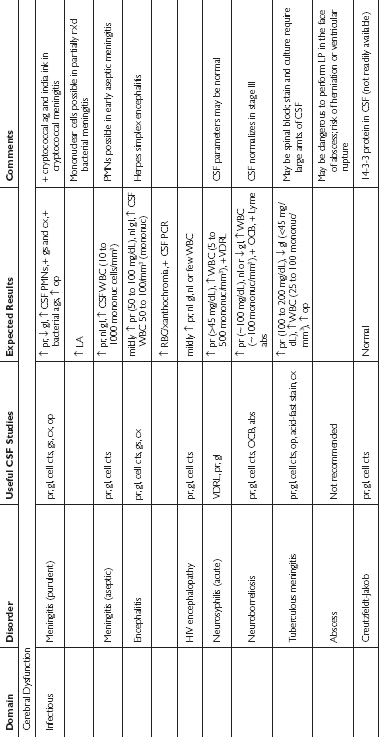
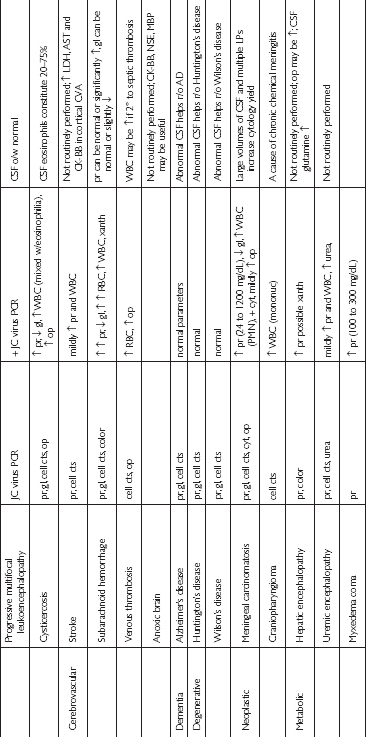
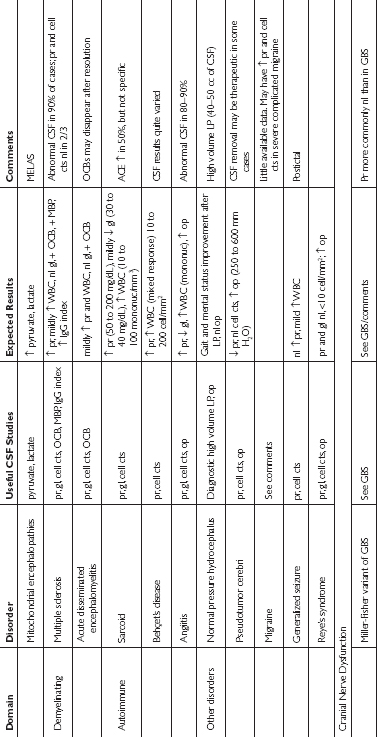
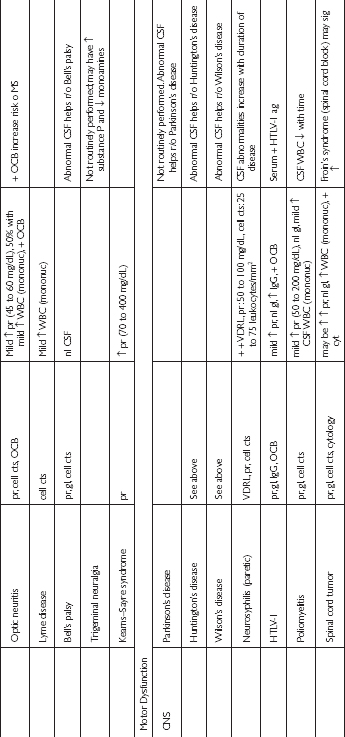
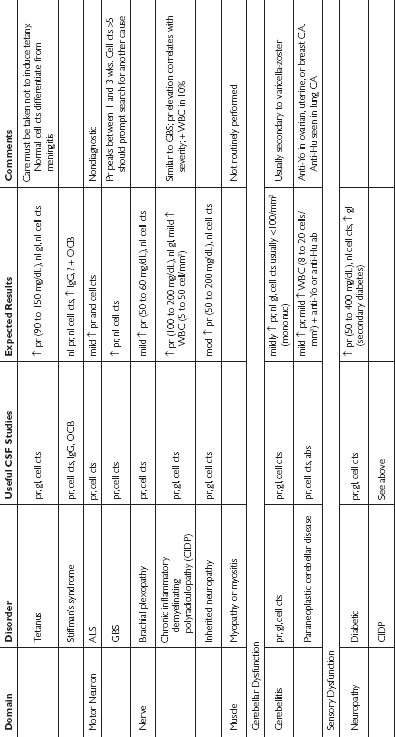
These typical findings, in combination with specific antigen, antibody, and polymerase chain reaction tests may help to reveal the origin of a CNS infection or disease. The tests that are ordered on the CSF should be guided by the suspected underlying cause of the patient’s illness. Recommended CSF studies based upon specific disorders are outlined in Table 10.2 below.

For bacterial meningitis, CSF Gram stain and culture are the diagnostic tests of choice. Blood culture may also help identify the causative organism. CSF viral culture is able to detect 14 to 24% of cases of viral meningitis. Tuberculous and fungal meningitis may be difficult to diagnose by routine CSF smear or culture. CSF culture is positive in 52 to 83% of cases of tuberculous meningitis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


