CHAPTER 13 CARDIOVASCULAR PATHOLOGY
INTRODUCTION

 protocols for management of transplant patients require repeated endomyocardial biopsies to assess rejection
protocols for management of transplant patients require repeated endomyocardial biopsies to assess rejection










DIAGNOSTIC ENDOMYOCARDIAL BIOPSY

 to avoid risk of perforation, specimens are taken from the right side of the interventricular septum
to avoid risk of perforation, specimens are taken from the right side of the interventricular septum






CARDIOMYOPATHIES





Table 13.1 Simplified classification of pediatric cardiomyopathies (Richardson et al 1996)
| Dilated cardiomyopathy |
| Hypertrophic cardiomyopathy |
| Restrictive cardiomyopathy |
| Arrhythmogenic right ventricular cardiomyopathy |
Histopathological features of cardiomyopathies on biopsy
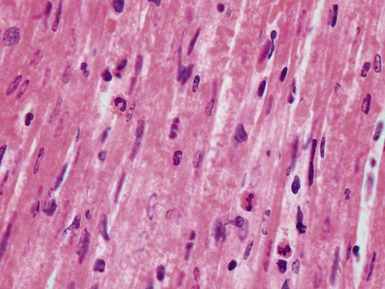
Dilated cardiomyopathy (Figs 13.1–13.4)





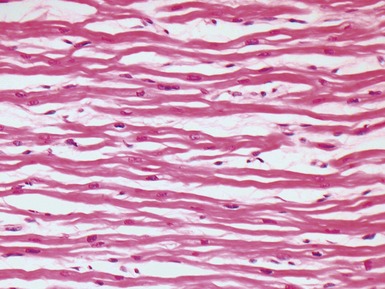
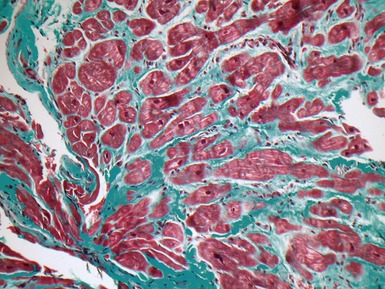
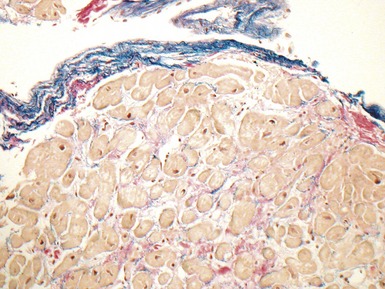
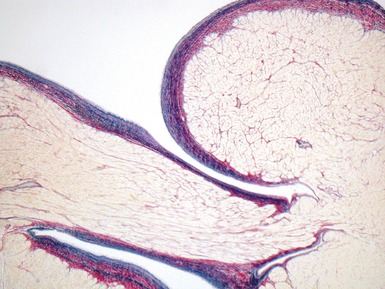
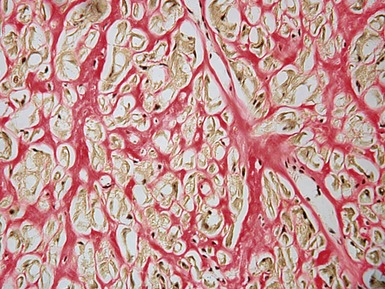
Fig 13.3 Photomicrograph of an endomyocardial biopsy from the same case as Fig 13.2. The myocytes show variation in size, as do their nuclei. There is mild interstitial fibrosis and the endocardium shows mild to moderate, fibroelastic thickening. (Elastic van Gieson)
Hypertrophic cardiomyopathy (Figs 13.5, 13.6)





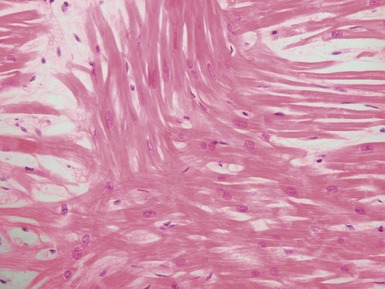
Fig 13.5 Photomicrograph of heart from an 11-year-old boy with hypertrophic cardiomyopathy. There is readily apparent myocyte disarray. Disarray is also usually evident at a macroscopic level where the muscle bundles are whorled, and also at the ultrastructural level where the myofilaments are disorganized.
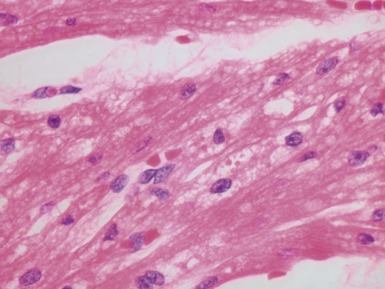
Table 13.2 Associations of myocyte disarray
| Familial hypertrophic cardiomyopathy |
| Restrictive cardiomyopathy |
| Normal heart near the insertion of the septum into the ventricular free walls |
| Congenital heart disease, particularly hypoplastic left heart |
| Previous biopsy site on endomyocardial biopsy (see section on post-transplant biopsy) |
| Adjacent to myocardial scars |
Restrictive cardiomyopathy

Other forms of cardiomyopathy





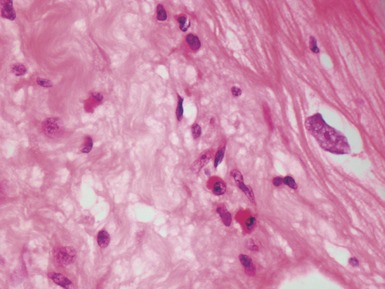
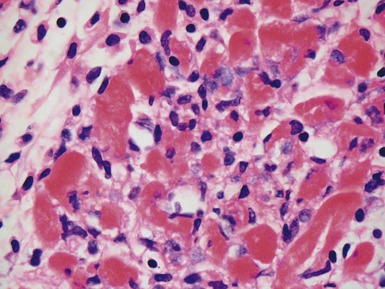
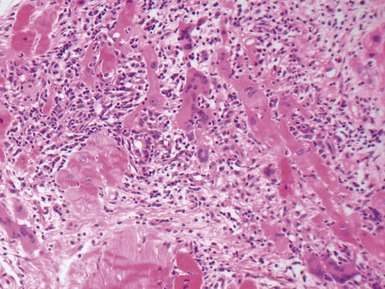
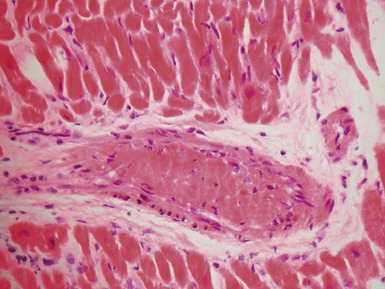
VIRAL MYOCARDITIS

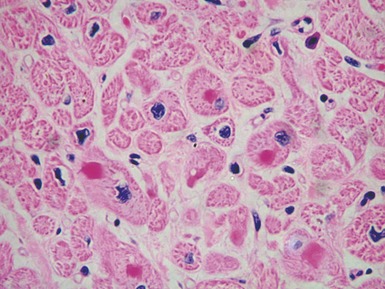
Histopathological features (Figs 13.9–13.13)



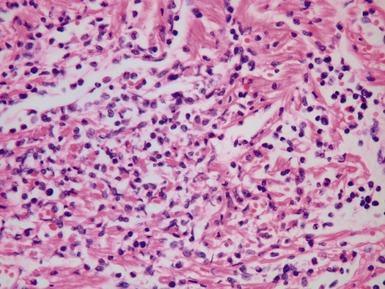
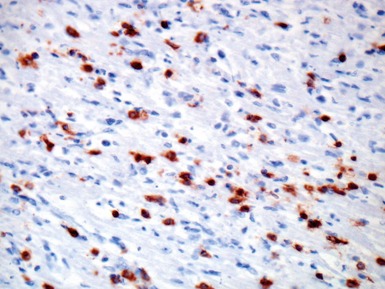
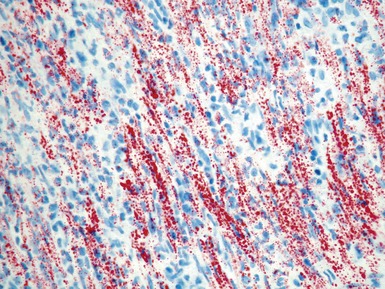
Fig 13.10 Same case as Fig 13.9 stained with anti-CD3 antibody. There are large numbers of positive T-cells in the myocardium.
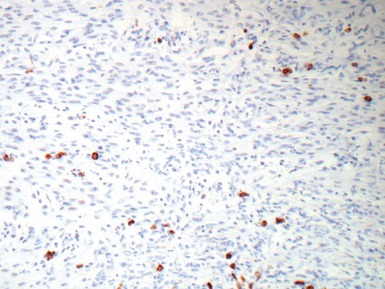
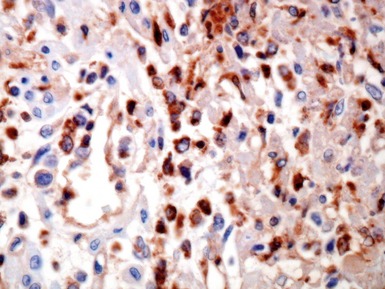
Fig 13.12 Same case as Fig 13.9 stained with antibody to CD68. There are large numbers of macrophages in the inflammatory cell infiltrate.








ASSESSMENT OF THE EXPLANTED HEART
INTRODUCTION


CARDIOMYOPATHIES IN THE EXPLANTED HEART









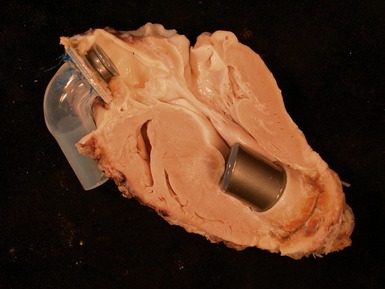
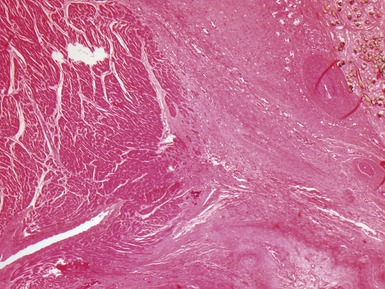
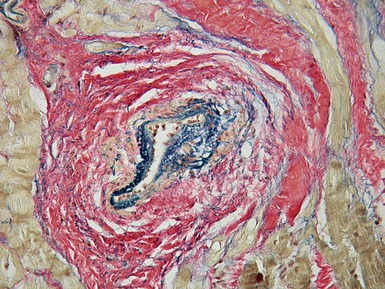
Fig 13.20 Same case as Fig 13.19, showing the cannula insertion site at the left ventricular apex. There is dense myocardial fibrosis. Dark flecks of dystrophic calcification are seen at the junction with the myocardium. Suture material is evident on the right. Inflammation is minimal in this case.
Histopathological features of cardiomyopathies in explanted hearts
Dilated cardiomyopathy
Macroscopic features (Fig 13.21)


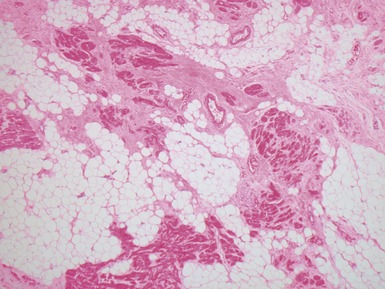
Microscopic features (Figs 13.22–13.24)




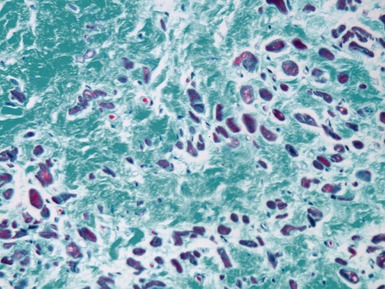
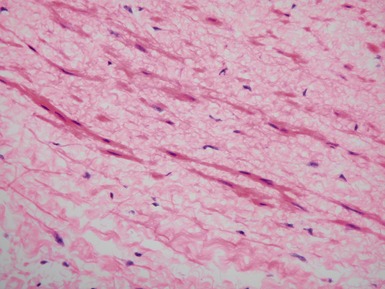
Fig 13.22 Photomicrograph of heart from a 4-year-old boy with dilated cardiomyopathy. Section of left ventricular myocardium of explanted heart shows extensive interstitial fibrosis with myocyte dropout. (Masson trichrome)
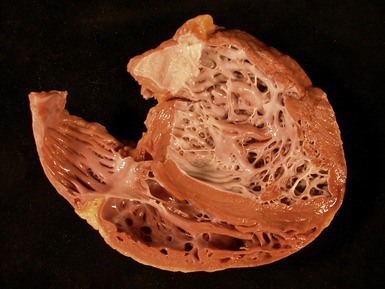
Hypertrophic cardiomyopathy
Macroscopic features (Fig 13.25)









MITOCHONDRIAL CARDIOMYOPATHIES






ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


