Chapter 410 Bronchopulmonary Dysplasia
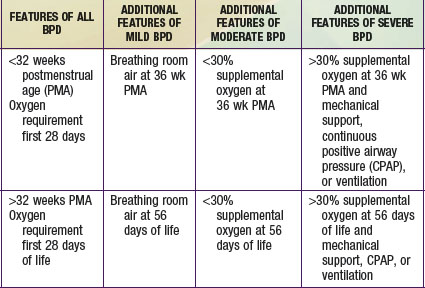
Bronchopulmonary dysplasia (BPD) is a syndrome characterized by signs and symptoms of chronic lung disease that originates in the neonatal period (Chapter 95). The pathogenesis of the lung disease was originally thought to arise from mechanical and oxidant injury to the airways and interstitium leading to edema, inflammation, and fibrosis with characteristic radiographic and pathologic stages. The pathogenesis of lung disease in the population of neonates <1000 g also includes the contribution of immature development of airway and vascular structures of the lung. This fact has led to a change in recognized radiographic, pathologic, and clinical findings in BPD and an evolution in its definition. An accepted definition includes an oxygen requirement for 28 days postnatally, and the disorder is graded as mild, moderate or severe on the basis of supplemental oxygen requirement and gestational age (see Table 410-1 on the Nelson Textbook of Pediatrics website at www.expertconsult.com  ).
).