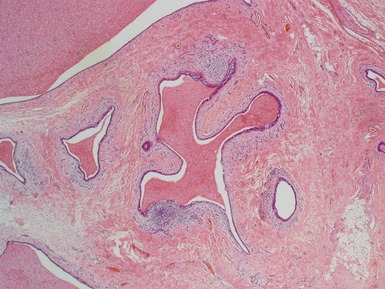
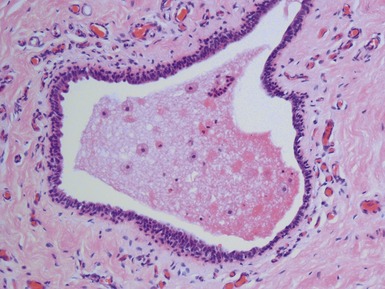
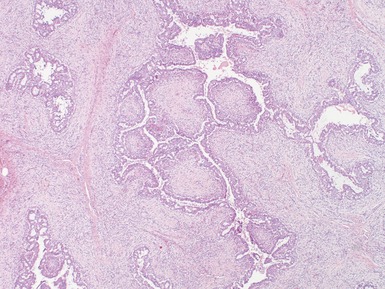
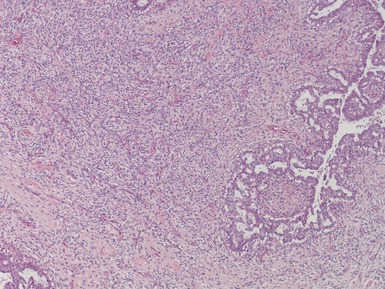
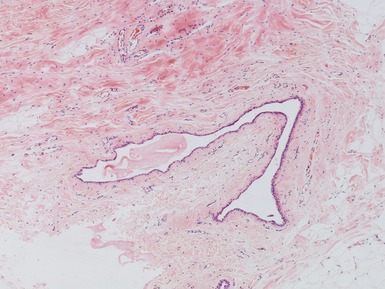
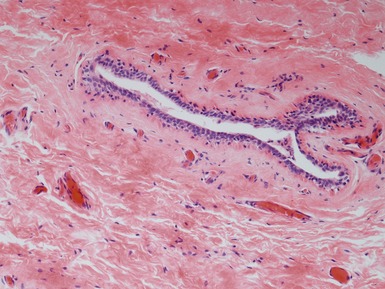
CHAPTER 5 BREAST AND FEMALE GENITAL TRACT PATHOLOGY Pediatric breast pathology Breast carcinoma Li–fraumeni syndrome Juvenile papillomatosis Fibrocystic change Fibrous mastopathy / diabetic mastopathy Fibroadenoma Phyllodes tumor Gynecomastia Virginal hypertrophy of the breast (macromastia) Supernumerary nipple Accessory breast tissue Genital tract pathology Ovarian germ cell tumors Mixed germ cell–stromal tumors Gonadoblastoma Small cell carcinoma of hypercalcemic type Ovarian sex-cord stromal tumors Ovarian cysts Streak ovary Massive ovarian edema Vulval lesions Clear cell adenocarcinoma of vagina/cervix Vaginal adenosis PEDIATRIC BREAST PATHOLOGY • Malignant disease is rare when present more likely to be secondary – especially ARMS • Mesenchymal tumors relatively much more common than in adulthood vascular lesions pseudoangiomatoid stromal hyperplasia – anastomosing slit-like spaces – CD34+ spindle cells, CD31− fibromatosis BREAST CARCINOMA • Rare in childhood • May affect both females and males very rare but reported in boys (Bhagwandeen et al 1999) • Secretory subtype most common (Longo et al 1999) ETV6-NTRK3 associated, same as IFS / CMN (Tognon et al 2002) low grade histological patterns – honeycomb / microcystic – solid – tubular ovoid cells with pale eosinophilic granular cytoplasm intracytoplasmic lumina • DPAS+ and AB+ mucin present • EMA+ • Good prognosis in children LI–FRAUMENI SYNDROME • Predisposition to multiple malignant tumors including sarcomas and carcinomas – occurring in children and adulthood · soft tissue sarcomas, adrenal cortical carcinoma and brain tumors in childhood · breast carcinoma in adulthood • Due to TP53 mutations JUVENILE PAPILLOMATOSIS • Mass lesion in breast • Usually young adults but reported in children including rarely infant boys • Increased risk of familial breast cancer • Unencapsulated macrocystic lesion with fibrous stroma (Figs 5.1, 5.2) multiple cysts dilated ducts with apocrine metaplasia duct ectasia sclerosing adenosis-like changes epithelial hyperplasia microcalcifications Fig. 5.1 Figs 5.1–5.2 Photomicrographs of child with juvenile papillomatosis, demonstrating duct ectasia with apocrine metaplasia and stromal sclerosis. FIBROCYSTIC CHANGE • Focal mass lesion in breast • Cystic change • Epithelial hyperplasia / metaplasia if atypical hyperplasia may be associated with increased risk of breast carcinoma FIBROUS MASTOPATHY / DIABETIC MASTOPATHY • Firm breast mass • Variably cellular spindle cells in collagenous stroma • Entrapped ducts / lobules • Lymphocytic infiltration with DM FIBROADENOMA (Figs 5.3, 5.4) • Painless firm breast nodule • May grow very large in adolescents (giant fibroadenoma) • Epithelial and mesenchymal components • Pericanalicular pattern stromal cells circumferentially surrounding ducts • Intracanalicular pattern ducts compressed into slit-like spaces • Variably cellular stromal component pediatric cases often more cellular myxoid or hyaline stromal change • Epithelial component variable hyperplastic and metaplastic changes pediatric cases often show epithelial proliferation • Note: Intramammary hamartoma may show similar clinical and macroscopic features circumscribed lesion admixture of all components of normal breast tissue – with or without superimposed secondary changes Fig. 5.3 Figs 5.3–5.4 Photomicrographs of child with a juvenile (giant) fibroadenoma, demonstrating cellular stroma which circumferentially surrounds ducts which show epithelial proliferation. PHYLLODES TUMOR • Biphasic lesion similar to fibroadenoma • Most are benign local recurrence and metastases reported in minority 2% mortality overall 10–20% local recurrence (Rajan et al 1998) • Mainly adults well-reported in childhood • Epithelial structures with surrounding stromal overgrowth stroma more cellular than fibroadenoma – especially hypercellular beneath epithelium – frankly malignant mesenchymal change may occur epithelium forms leaf-like areas – epithelial hyperplasia / metaplasia • Predictors of malignant behavior based on: degree of hypercellularity pleomorphism mitotic count stromal overgrowth – poor prediction of behavior in individual cases local relapse associated with – positive margins – fibroproliferation in surrounding tissue – necrosis (Barrio et al 2007) GYNECOMASTIA • Enlargement of the male breast ductular system Epidemiology • Males • In childhood may occur in neonates and adolescents Clinical features • Bilateral but often asymmetric breast enlargement Histopathological features (Figs 5.5, 5.6) • Circumscribed area of ducts with surrounding stroma • Stroma may be myxoid, with scattered inflammatory cells hyalinization with progression • Epithelium usually bland ectasia, metaplasia and hyperplasia may occur Fig. 5.5 Figs 5.5–5.6 Photomicrographs of breast lesions from a boy with gynecomastia, demonstrating ductular structures within a bland hyalinized stroma. Differential diagnoses and pitfalls • Always consider possible underlying endocrinopathies VIRGINAL HYPERTROPHY OF THE BREAST (MACROMASTIA) • Gynecomastia-like changes but in female breast around puberty • Proliferation of ducts within hypocellular stroma may show pseudoangiomatous hyperplasia-like stromal changes stroma less cellular than fibroadenoma SUPERNUMERARY NIPPLE • Pigmented macule on milk line rarely more ‘ectopic’ position • Histologically features of normal nipple • Wide range of tumor may develop usually in adults ACCESSORY BREAST TISSUE Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: BONE PATHOLOGY HEAD AND NECK PATHOLOGY RENAL PATHOLOGY TUMORS AND TUMOR-LIKE LESIONS Stay updated, free articles. Join our Telegram channel Join Tags: Diagnostic Pediatric Surgical Pathology Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on BREAST AND FEMALE GENITAL TRACT PATHOLOGY Full access? Get Clinical Tree
CHAPTER 5 BREAST AND FEMALE GENITAL TRACT PATHOLOGY Pediatric breast pathology Breast carcinoma Li–fraumeni syndrome Juvenile papillomatosis Fibrocystic change Fibrous mastopathy / diabetic mastopathy Fibroadenoma Phyllodes tumor Gynecomastia Virginal hypertrophy of the breast (macromastia) Supernumerary nipple Accessory breast tissue Genital tract pathology Ovarian germ cell tumors Mixed germ cell–stromal tumors Gonadoblastoma Small cell carcinoma of hypercalcemic type Ovarian sex-cord stromal tumors Ovarian cysts Streak ovary Massive ovarian edema Vulval lesions Clear cell adenocarcinoma of vagina/cervix Vaginal adenosis PEDIATRIC BREAST PATHOLOGY • Malignant disease is rare when present more likely to be secondary – especially ARMS • Mesenchymal tumors relatively much more common than in adulthood vascular lesions pseudoangiomatoid stromal hyperplasia – anastomosing slit-like spaces – CD34+ spindle cells, CD31− fibromatosis BREAST CARCINOMA • Rare in childhood • May affect both females and males very rare but reported in boys (Bhagwandeen et al 1999) • Secretory subtype most common (Longo et al 1999) ETV6-NTRK3 associated, same as IFS / CMN (Tognon et al 2002) low grade histological patterns – honeycomb / microcystic – solid – tubular ovoid cells with pale eosinophilic granular cytoplasm intracytoplasmic lumina • DPAS+ and AB+ mucin present • EMA+ • Good prognosis in children LI–FRAUMENI SYNDROME • Predisposition to multiple malignant tumors including sarcomas and carcinomas – occurring in children and adulthood · soft tissue sarcomas, adrenal cortical carcinoma and brain tumors in childhood · breast carcinoma in adulthood • Due to TP53 mutations JUVENILE PAPILLOMATOSIS • Mass lesion in breast • Usually young adults but reported in children including rarely infant boys • Increased risk of familial breast cancer • Unencapsulated macrocystic lesion with fibrous stroma (Figs 5.1, 5.2) multiple cysts dilated ducts with apocrine metaplasia duct ectasia sclerosing adenosis-like changes epithelial hyperplasia microcalcifications Fig. 5.1 Figs 5.1–5.2 Photomicrographs of child with juvenile papillomatosis, demonstrating duct ectasia with apocrine metaplasia and stromal sclerosis. FIBROCYSTIC CHANGE • Focal mass lesion in breast • Cystic change • Epithelial hyperplasia / metaplasia if atypical hyperplasia may be associated with increased risk of breast carcinoma FIBROUS MASTOPATHY / DIABETIC MASTOPATHY • Firm breast mass • Variably cellular spindle cells in collagenous stroma • Entrapped ducts / lobules • Lymphocytic infiltration with DM FIBROADENOMA (Figs 5.3, 5.4) • Painless firm breast nodule • May grow very large in adolescents (giant fibroadenoma) • Epithelial and mesenchymal components • Pericanalicular pattern stromal cells circumferentially surrounding ducts • Intracanalicular pattern ducts compressed into slit-like spaces • Variably cellular stromal component pediatric cases often more cellular myxoid or hyaline stromal change • Epithelial component variable hyperplastic and metaplastic changes pediatric cases often show epithelial proliferation • Note: Intramammary hamartoma may show similar clinical and macroscopic features circumscribed lesion admixture of all components of normal breast tissue – with or without superimposed secondary changes Fig. 5.3 Figs 5.3–5.4 Photomicrographs of child with a juvenile (giant) fibroadenoma, demonstrating cellular stroma which circumferentially surrounds ducts which show epithelial proliferation. PHYLLODES TUMOR • Biphasic lesion similar to fibroadenoma • Most are benign local recurrence and metastases reported in minority 2% mortality overall 10–20% local recurrence (Rajan et al 1998) • Mainly adults well-reported in childhood • Epithelial structures with surrounding stromal overgrowth stroma more cellular than fibroadenoma – especially hypercellular beneath epithelium – frankly malignant mesenchymal change may occur epithelium forms leaf-like areas – epithelial hyperplasia / metaplasia • Predictors of malignant behavior based on: degree of hypercellularity pleomorphism mitotic count stromal overgrowth – poor prediction of behavior in individual cases local relapse associated with – positive margins – fibroproliferation in surrounding tissue – necrosis (Barrio et al 2007) GYNECOMASTIA • Enlargement of the male breast ductular system Epidemiology • Males • In childhood may occur in neonates and adolescents Clinical features • Bilateral but often asymmetric breast enlargement Histopathological features (Figs 5.5, 5.6) • Circumscribed area of ducts with surrounding stroma • Stroma may be myxoid, with scattered inflammatory cells hyalinization with progression • Epithelium usually bland ectasia, metaplasia and hyperplasia may occur Fig. 5.5 Figs 5.5–5.6 Photomicrographs of breast lesions from a boy with gynecomastia, demonstrating ductular structures within a bland hyalinized stroma. Differential diagnoses and pitfalls • Always consider possible underlying endocrinopathies VIRGINAL HYPERTROPHY OF THE BREAST (MACROMASTIA) • Gynecomastia-like changes but in female breast around puberty • Proliferation of ducts within hypocellular stroma may show pseudoangiomatous hyperplasia-like stromal changes stroma less cellular than fibroadenoma SUPERNUMERARY NIPPLE • Pigmented macule on milk line rarely more ‘ectopic’ position • Histologically features of normal nipple • Wide range of tumor may develop usually in adults ACCESSORY BREAST TISSUE Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: BONE PATHOLOGY HEAD AND NECK PATHOLOGY RENAL PATHOLOGY TUMORS AND TUMOR-LIKE LESIONS Stay updated, free articles. Join our Telegram channel Join Tags: Diagnostic Pediatric Surgical Pathology Expert Consult Jun 18, 2016 | Posted by admin in PEDIATRICS | Comments Off on BREAST AND FEMALE GENITAL TRACT PATHOLOGY Full access? Get Clinical Tree