Fig. 14.1
The Barbed sutur
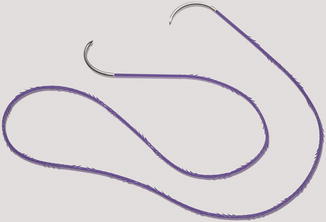
Fig. 14.2
Barbed sutur with 2 needles
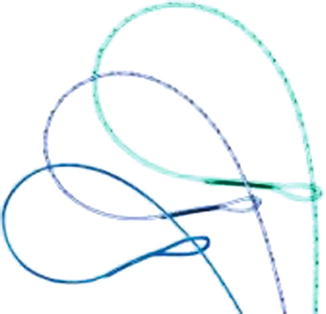
Fig. 14.3
Barbed sutur with loop
Various combinations of suture size, length, needle type, and monofilament material (including absorbable, delayed absorbable, and permanent options) are available in both bidirectional and unidirectional form. It is important to review the grading system employed by the barbed suture manufacturer to ensure a suture of sufficient strength is selected (Greenberg 2010). Some barbed suture (for example, QuillTM or STRATAFIXTM (Ethicon, Somerville NJ) suture)) is size-rated prior to the barbs being cut, and is equivalent in strength to smooth suture of one size smaller. Other barbed suture (for example, V-LocTM) is size-rated after barbs are cut into the material and of equal strength as the same size smooth suture.
14.3 Tips for Use in Gynecologic Laparoscopy
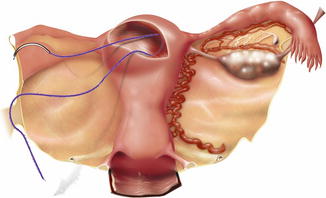
Barbed suture may be particularly useful for closure of the vaginal cuff at the time of total laparoscopic hysterectomy or trachelectomy. Several options for closure technique exist, depending on whether unidirectional or bidirectional barbed suture is chosen. Utilizing unidirectional suture, the surgeon may begin at one apex, anchor the suture via the loop on the trailing end, and move toward the other apex with continuous nonlocking bites. Once the full length of the vaginal incision has been re-approximated, it may be helpful to take several back bites toward the midline in order to further anchor the suture. Additionally, one may choose to utilize two separate unidirectional sutures, beginning at each apex with an individual suture, suturing toward the midline and taking overlapping bites in the middle.
When employing bidirectional barbed suture, the surgeon may begin in the middle of the incision, taking care to pull the suture through the tissue until resistance is met, indicating the mid-point of the suture where the barbs change direction (Fig. 14.4). One needle end of the suture is used to close toward the left of the incision, and the other to close toward the right (Figs. 14.5 and 14.6). Again, backbites may be helpful after completing closure to enhance suture anchoring. If a double-layer closure is desired, the bidirectional suturing is begun by placing the first bite at one apex, pulling the suture through until the mid-point resistance is met, and suturing in a continuous fashion toward the other apex. The second half of the suture is then utilized to work in the same direction and create an imbricating layer. Favorable outcomes have been reported with the use of barbed suture for vaginal cuff closure, including decreased incidence of cuff dehiscence, postoperative vaginal bleeding, formation of granulation tissue, and vaginal cuff cellulitis (Siedhoff et al. 2011).
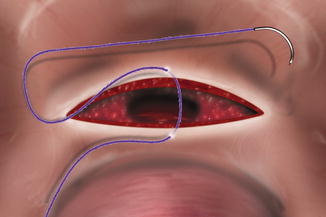

Fig. 14.4
Start in middle
Fig. 14.5
Sutur left
Fig. 14.6
Sutur right with the other needle
During laparoscopic myomectomy, hysterotomy closure is also greatly facilitated by use of barbed suture. If a surgeon chooses unidirectional barbed suture, the defect may be closed in standard multilayer fashion by continuous suturing techniques. With bidirectional barbed suture, the first half of the suture is used to close the deepest layer, with the second half utilized for closure of the more superficial layers (Figs. 14.7, 14.8 and 14.9). It may be helpful to tack the nonworking needle to the anterior abdominal wall when using a long bidirectional suture in order to avoid tangling of the suture ends (Einarsson and Greenberg 2009). The use of barbed suture for laparoscopic myomectomy has demonstrated benefits including facilitating ease of a complex suturing task and decreased time required for hysterotomy closure, with variable findings regarding reduction in blood loss (Einarsson and Greenberg 2009; Allesandri et al. 2010; Angioli et al. 2012).