Chapter 7 Antepartum Care
PRECONCEPTION AND PRENATAL CARE, GENETIC EVALUATION AND TERATOLOGY, AND ANTENATAL FETAL ASSESSMENT
 Preconception Care
Preconception Care
Several models of preconception care have been developed. Major components of preconception care include risk assessment, health promotion, and medical and psychosocial interventions and follow-up, as summarized in Table 7-1. There is currently no consensus on the timing of preconception care, probably because there are different ideas about what preconception care should be or do. For some, preconception care means a single prepregnancy checkup a few months before couples attempt to conceive. A single visit, however, may be too little too late to address some problems (e.g., promoting smoking cessation or healthy weight) and will miss those pregnancies that are unintended at the time of conception (about half of all pregnancies in the United States). For others, preconception care means all well-woman care, from prepubescence to menopause. In practice, however, asking providers to squeeze more into an already hurried routine visit may not be feasible, and some components (e.g., genetic screening or laboratory testing) may not be indicated for every woman at every visit.
TABLE 7-1 ELEMENTS OF PRECONCEPTION COUNSELING AND CARE
| Major Components of Preconception Care | Risk Assessment |
|---|---|
| Reproductive life plan | Ask your patient if she plans to have any (more) children and how long she plans to wait until she (next) becomes pregnant. Help her develop a plan to achieve those goals. |
| Past reproductive history | Review prior adverse pregnancy outcomes, such as fetal loss, birth defects, low birth weight, and preterm birth, and assess ongoing biobehavioral risks that could lead to recurrence in a subsequent pregnancy. |
| Past medical history | Ask about past medical history such as rheumatic heart disease, thromboembolism, or autoimmune diseases that could affect future pregnancy. Screen for ongoing chronic conditions such as hypertension and diabetes. |
| Medications | Review current medication use. Avoid category X drugs and most category D drugs unless potential maternal benefits outweigh fetal risks (see Box 7-1). Review use of over-the-counter medications, herbs, and supplements. |
| Infections and immunizations | Screen for periodontal, urogenital, and sexually transmitted infections as indicated. Discuss TORCH (toxoplasmosis, other, rubella, cytomegalovirus, and herpes) infections and update immunization for hepatitis B, rubella, varicella, Tdap (combined tetanus, diphtheria, and pertussis), human papillomavirus, and influenza vaccines as needed. |
| Genetic screening and family history | Assess risk for chromosomal or genetic disorders based on family history, ethnic background, and age. Offer cystic fibrosis screening. Discuss management of known genetic disorders (e.g., phenylketonuria, thrombophilia) before and during pregnancy. |
| Nutritional assessment | Assess anthropometric (body mass index), biochemical (e.g., anemia), clinical, and dietary risks. |
| Substance abuse | Ask about smoking, alcohol, drug use. Use T-ACE (tolerance, annoyed, cut down, eye opener) or CAGE (cut-down, annoyed, guilty, eye-opener) questions to screen for alcohol and substance abuse. |
| Toxins and teratogens | Review exposures at home, neighborhood, and work. Review Material Safety Data Sheet and consult local Teratogen Information Service as needed. |
| Psychosocial concerns | Screen for depression, anxiety, intimate-partner violence, and major psychosocial stressors. |
| Physical examination | Focus on periodontal, thyroid, heart, breasts, and pelvic examination. |
| Laboratory tests | Check complete blood count, urinalysis, type and screen, rubella, syphilis, hepatitis B, HIV, cervical cytology; screen for gonorrhea, chlamydia, and diabetes in selected populations. Consider thyroid-stimulating hormone. |
| Major Components of Preconception Care | Health promotion |
| Family planning | Promote family planning based on a woman’s reproductive life plan. For women who are not planning on getting pregnant, promote effective contraceptive use and discuss emergency contraception. |
| Healthy weight and nutrition | Promote healthy prepregnancy weight through exercise and nutrition. Discuss macronutrients and micronutrients, including 5-a-day and daily intake of multivitamin containing folic acid. |
| Health behaviors | Promote such health behaviors as nutrition, exercise, safe sex, effective use of contraception, dental flossing, and use of preventive health services. Discourage risk behaviors such as douching, nonuse of seat belt, smoking, and alcohol and substance abuse. |
| Stress resilience | Promote healthy nutrition, exercise, sleep, and relaxation techniques; address ongoing stressors such as intimate partner violence; identify resources to help patient develop problem-solving and conflict resolution skills, positive mental health, and relational resilience. |
| Healthy environments | Discuss household, neighborhood, and occupational exposures to metals, organic solvents, pesticides, endocrine disruptors, and allergens. Give practical tips such as how to reduce exposures during commuting or picking up dry cleaning. |
 Prenatal Care
Prenatal Care
THE FIRST PRENATAL VISIT
Standardized forms have been developed to facilitate overall prenatal risk assessment. One such system is the Problem Oriented Prenatal Risk Assessment System, or POPRAS (www.POPRAS.com).
Prenatal laboratory testing should be undertaken as outlined in Table 7-1, if not done during preconception care. Screening for and treating asymptomatic bacteriuria significantly reduces the risk for pyelonephritis and preterm delivery.
 Confirming Pregnancy and Determining Viability
Confirming Pregnancy and Determining Viability
TYPES OF SPONTANEOUS ABORTION
ETIOLOGY
General Maternal Factors
Three medical disorders are commonly linked to spontaneous abortion: (1) diabetes mellitus, (2) hypothyroidism, and (3) systemic lupus erythematosus (SLE). The evidence linking diabetes mellitus with spontaneous abortion is not conclusive, and severe hypothyroidism is more often associated with disordered ovulation than spontaneous abortion. Up to 40% of clinical pregnancies are lost in women with SLE, and such patients have an increased risk for pregnancy loss before developing the clinical stigmata of the disease (see Chapter 16).
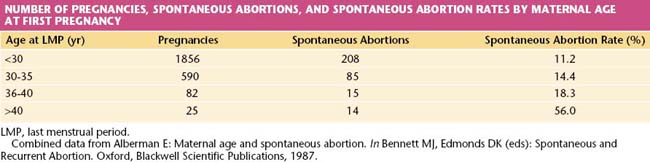
The risk for abortion increases with maternal age (Table 7-2). If a live fetus is demonstrated by ultrasonography at 8 weeks’ gestational age, however, fewer than 2% will abort spontaneously when the mother is younger than 30 years of age. If she is older than 40 years, the risk exceeds 10%, and it may be as high as 50% at age 45 years. The probable explanation is the increased incidence of chromosomally abnormal conceptus in older women.
Immunologic Factors
A successful pregnancy depends on a number of immunologic factors that allow the host (mother) to retain an antigenically foreign product (fetus) without rejection taking place (see Chapter 6). The precise mechanism of this immunologic anomaly is not fully understood, but the immunologic functioning of some women, particularly those who abort recurrently, is different from that of women who carry pregnancies to term. The immunologic relationship between male and female in such a couple may be regarded as abnormal, and in some instances, treatment of this condition may result in a successful pregnancy.
MANAGEMENT
Recurrent Abortion
More than half of couples with recurrent losses will have normal findings during an evaluation. When a specific etiologic factor is found, appropriate management often leads to reproductive success. Many of the congenital abnormalities of the uterus can now be diagnosed using pelvic ultrasonography and may no longer require laparotomy for repair. Cervical incompetence is managed by the placement of a cervical suture (cerclage) at the level of the internal os, and this suture is best placed in the first trimester, after a live fetus has been demonstrated on ultrasonography. The effectiveness of prophylactic cervical cerclage (see Chapters 17 and 19) in preventing recurrent loss from cervical incompetence has not been conclusively established.
 Estimating Gestational Age and Date of Confinement
Estimating Gestational Age and Date of ConfinementStay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


