18 Anaphylaxis
Etiology and Pathogenesis
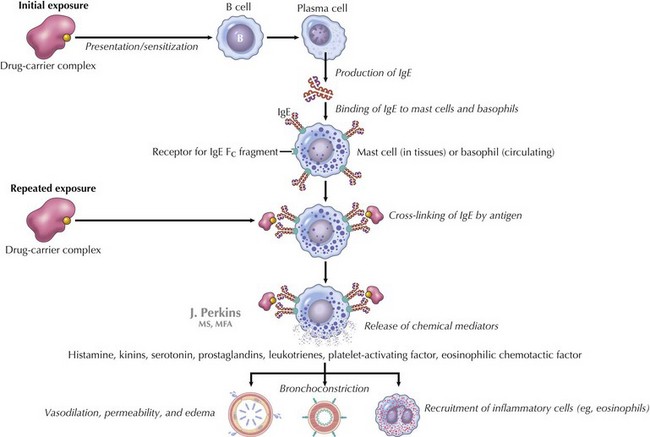
IgE-mediated anaphylaxis, a type I hypersensitivity reaction, is the most understood form of anaphylaxis (Figure 18-1). A person is exposed to an antigen, and upon reexposure, cross-linkage of IgE occurs followed by an immediate release of potent mediators from tissue mast cells and peripheral basophils. These mediators include histamine, leukotrienes, nitric oxide, and neutral proteases, which all lead to vasodilatation, increased vascular permeability, bronchoconstriction, and additional inflammation. At times, the reaction occurs with the first known exposure.
Clinical Presentation
Patients with anaphylaxis may have different clinical manifestations (Table 18-1). Anaphylaxis is often underdiagnosed or misdiagnosed because of clinicians’ failure to recognize symptoms. There has been a recent attempt to standardize the diagnostic criteria to help clinicians to better recognize anaphylaxis (Box 18-1 and Figure 18-2). Approximately 90% of children with allergic reactions have skin manifestations, which include hives, angioedema (see Chapter 20, Figures 20-1 and 20-2), pruritus, or flushing. Although the remainder may not have skin involvement, they are still having a reaction, and that reaction may be more severe than those that occur with skin findings present. Tongue and throat swelling, dysphagia, and choking are manifestations of upper airway edema. Lower respiratory tract symptoms, such as coughing and wheezing, are the next most common symptoms. Vomiting, diarrhea, and abdominal pain are often seen, especially in food-induced anaphylaxis. Cardiovascular manifestations include tachycardia, hypotension, shock, and (rarely) bradycardia. Children may also be lethargic, and some have described a “feeling of impending doom.”
Table 18-1 Signs and Symptoms of Anaphylactic Reactions
| Systems | Signs and Symptoms |
|---|---|
| Cutaneous | |
| Respiratory | Upper Respiratory |
| Lower Respiratory | |
| Cardiovascular | |
| Gastrointestinal | |
| Neurologic |
Box 18-1
Proposed Diagnostic Criteria for Classic Anaphylaxis
Need Any One of Three Criteria to Qualify As Anaphylaxis
Skin mucosal tissue (e.g., hives; generalized itch or flush; swollen lips, tongue, or uvula)
Airway compromise (e.g., dyspnea, wheeze or bronchospasm, stridor, reduced PEF)
Hypotension or associated symptoms (e.g., hypotonia, syncope)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


