125 Acne
Etiology And Pathogenesis
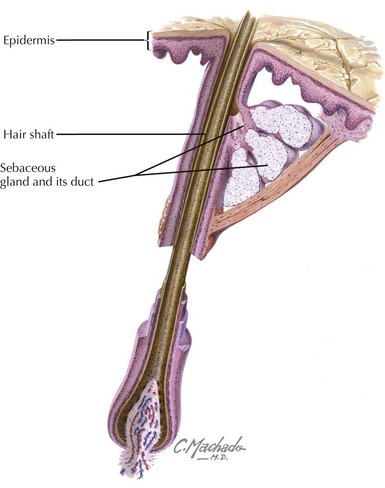
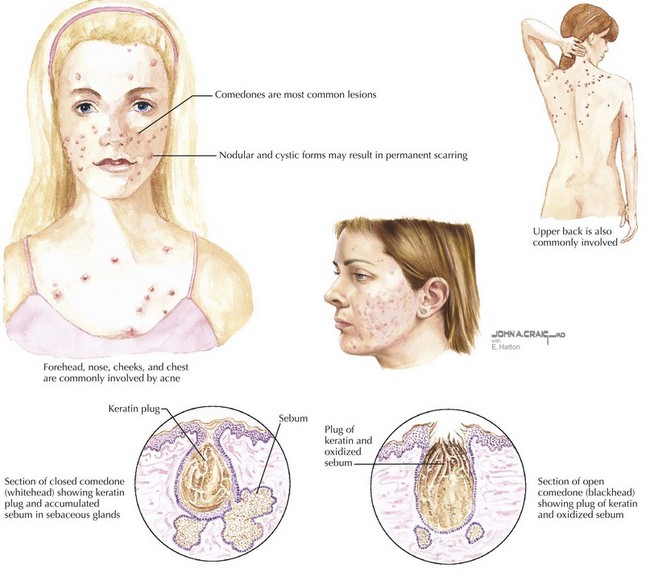
An appreciation of the pathogenesis of acne facilitates a better understanding of targeted treatments. Acne develops in the pilosebaceous unit (Figure 125-1). There are four primary factors involved: abnormal keratinization, increased sebum production, proliferation of Propionibacterium acnes bacteria, and inflammation. With the onset of adrenarche, there is an increase in androgen production and a resultant increase in sebum secretion. Each sebaceous gland has a different threshold of androgen sensitivity, effecting an individually unique response to puberty. Simultaneously, there is increased proliferation of keratinocytes and decreased desquamation. The accumulation of sebum and keratinocytes leads to the formation of the microcomedo, the precursor to acne lesions. P. acnes, a normal skin inhabitant, thrives in this lipid-rich environment. The organisms release chemotactic factors, setting up an inflammatory response. Depending on the contribution of each primary factor, a microcomedo can evolve into a closed comedo (whitehead), open comedo (blackhead) (Figure 125-2), or an inflammatory pustule, papule, or nodule if the sebum, keratin, and microorganisms, with the accumulation of inflammatory cells, rupture into the dermis.
Clinical Presentation
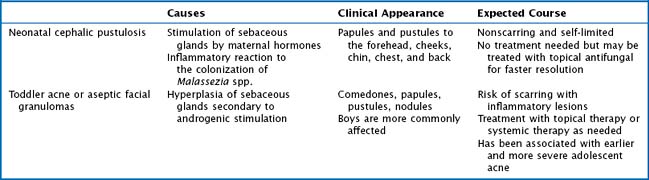
Acne is a disease that can be seen in the first year of life, early childhood, the prepubertal period, and puberty. Neonatal cephalic pustulosis, formerly referred to as neonatal acne, appears in the first 3 months after birth and usually resolves in 1 to 3 months. In neonates, it is extremely important to exclude other bacterial, viral, or fungal causes, but a physician should also consider milia, erythema toxicum neonatorum, transient neonatal pustulosis, and sebaceous gland hyperplasia. Infantile or toddler acne is less common and usually presents between 3 and 6 months of life and can last 1 to 2 years. This is not typically associated with precocious puberty or a hormonal imbalance but needs to be considered in conjunction with a thorough history and physical examination. See Table 125-1 for a comparison of acne seen in neonates and toddlers. Acne can present in any location where there are sebaceous glands. In addition to the face, it is frequently found on the neck, upper chest, shoulders, and back (see Figure 125-2). There are multiple classification systems used to talk about acne, but a description of the lesions and their locations is most helpful. The resolution of acne may leave postinflammatory changes that usually resolve themselves but may take weeks to months, especially in darker pigmented patients. Moderate and severe acne can leave permanent scars.
The diagnosis of acne is relatively straightforward. Typical acne includes comedones, papules, pustules, and nodules in the distribution of the face, upper back, and chest. Acne that begins at an abnormal age, particularly severe acne, acne accompanied by an abnormal growth history or virilization, or acne that is recalcitrant to treatment, should be further evaluated. The physician may want to consider an underlying disorder, such as premature adrenarche, precocious puberty, Cushing’s syndrome, congenital adrenal hyperplasia, and gonadal or adrenal tumors, or an alternative diagnosis if the lesions are not typical (Box 125-1). Perioral dermatitis and facial angiofibromas are shown in Figure 125-3.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


