Fig. 5.1
A right rudimentary horn with a normal developed left uterus. There is pelvic endometriosis
The key to ultrasound diagnosis of rudimentary horn and hemi-uterus is to display the uterine shape on the coronal plane and to identify whether there is asymmetrical uterine appearance. The fundus of the uterus appears narrow, with its endometrium deviating to one side like a lancet-shaped endometrial cavity. Further examination should be done to find the rudimentary horn. If a rudimentary horn is found, the presence of endometrium in the rudimentary horn cavity and its connection with the normal hemi-uterus should be defined. Depending on whether the rudimentary horn is functional or not, further subtypes are defined [3, 5]. A rudimentary horn without functional cavity or retained blood due to hemorrhage can easily be misdiagnosed as a uterine fibroid or degenerative fibroid, but 3D ultrasound however can display the uterine morphology for identification. Hysterosalpingography (HSG) is helpful in the diagnosis of rudimentary horn, with its typical banana sign. Here, the contrast medium enters further into the fallopian tube on one side. If the rudimentary horn and the developed hemi-uterus are connected, the contrast medium will be seen entering into the rudimentary horn. However, if hysterosalpingography does not show a rudimentary horn, diagnosis cannot be assumed because of a lack of connection between the rudimentary horn and the developed hemi-uterus [3]. MRI can clearly show whether the rudimentary horn has an endometrium or not and whether it is connected with the uterine cavity of the developed hemi-uterus; therefore, MRI can clearly diagnose the types of rudimentary horn [6]. CT angiography can also clearly reveal the blood supply of the rudimentary horn. However, ultrasound saline hysterosalpingogram and hysteroscopy examination remain the standard assessment and diagnostic method of uterine anomalies [7]. Those with obstructed menstrual flow should be alerted for possible pelvic endometriosis. Blood CA125 can help diagnose the coexistence of endometriosis.
In view of the common origin of the urinary system and the reproductive system during their embryonic development, patients who are suspected of having uterine malformation should undergo conventional ultrasound or MRI examinations to check for the status of the kidneys. This may, for example, be found on the same side as the rudimentary horn; there is an absence of an ipsilateral kidney, an ectopic kidney, a horseshoe kidney, or other cystic renal dysplasia, etc. Patients with type U5 aplastic uterus are often associated with other malformations, such as vaginal anomalies or MRHK syndrome [4].
A fertilized egg can embed in the rudimentary horn, grow, and develop into a rudimentary horn pregnancy (Fig. 5.2). There are four possible mechanisms of pregnancy:
Fig. 5.2
Laparoscopic visualization of rudimentary horn pregnancy
1.
Sperms from the uterine cavity of the developed uterus pass through a small communicating tube joining the rudimentary horn, then to its fallopian tube. Pregnancy in the rudimentary horn will occur after they fertilize the egg ovulated from the ovary on the side of the rudimentary horn. The fertilized egg then embeds in the uterine cavity of the rudimentary horn.
2.
Sperms travel from the uterine cavity and out of the fallopian tube of the developed uterus, through the peritoneal cavity to the fallopian tube of the rudimentary horn. This will result in pregnancy after they fertilize the egg ovulated from the ovary. The fertilized egg subsequently embeds in the cavity of the rudimentary horn.
3.
Sperms and eggs from the developed side travel through the peritoneal cavity to the fallopian tube of the rudimentary horn, resulting in pregnancy. The fertilized egg embeds in the cavity of the rudimentary horn.
4.
The fertilized egg travels out from the fallopian tube of the developed side, via the peritoneal cavity to the fallopian tube of the rudimentary horn, and embeds and develops inside the rudimentary horn.
The survival rate of the fetus in rudimentary horn pregnancy is only 0–13 %. Rudimentary horn pregnancy is generally asymptomatic in the early stage. Fifty percent rudimentary horn pregnancy will rupture spontaneously, of which more than 80 % ruptures in rudimentary horn pregnancy occurred in midtrimester pregnancy, far later than ruptured tubal pregnancy.
At midtrimester pregnancy, because of the thin uterine wall of the undeveloped rudimentary horn, rupture typically occurs spontaneously, causing sudden onset of severe abdominal pain and hemorrhagic shock. This will endanger the life of the pregnant patient, with a mortality rate of 0.5–23 %.
When rudimentary horn communicates with the hemi-uterus, rudimentary horn pregnancy has similar symptoms as a tubal ectopic pregnancy, with a history of amenorrhea, abdominal pain, and vaginal bleeding. However, 80 % of rudimentary horn pregnancies occur in non-communicating rudimentary horns. The symptoms of these rudimentary horn pregnancies are similar to those in normal pregnancy without vaginal bleeding, but they will rupture at a later time.
Mostly at 12–26 weeks of pregnancy, they present with complete or incomplete uterine rupture, causing severe internal bleeding. When rudimentary horn pregnancy enlarges the horn, one should be aware of the risk of torsion of a rudimentary uterine horn pregnancy [8]. If the rudimentary horn has no functional uterine cavity, it will not result in rudimentary horn pregnancy; rarely, however, a tubal pregnancy on the side of rudimentary horn can still be possible.
The diagnostic criterion for rudimentary horn pregnancy is to use the round ligament as a guide. If the fetal sac is located medial to the round ligament attachment, it is a rudimentary horn pregnancy. If it is located lateral to the round ligament attachment, it is a tubal pregnancy. As a patient with rudimentary horn may have a normal vagina and cervix, but a small rudimentary horn, it is difficult to make a diagnosis based solely on bimanual pelvic examination before pregnancy. Patients with a history of infertility, premature labor, and spontaneous miscarriage should undergo both ultrasound scan and MRI to exclude uterine anomalies and ectopic uterine pregnancy. Three-dimensional ultrasound on rudimentary uterine pregnancy is a particularly effective diagnostic tool. The key points of 3D ultrasound diagnosis are the absence of a cervix in the pregnant uterus and presence of another nonpregnant uterus. Then the application of 3D imaging can observe the morphology of the hemi-uterus cavity, confirming the absence of a pregnancy sac. The endometrium is like a lancet pointing to one side of its uterine horn. In the lower end of the uterus, there is a tissue mass echo (i.e., rudimentary uterine horn); visible within it is a pregnancy sac or embryo. But the pregnancy sac and cervix are not connected. These findings can be diagnosed as rudimentary horn pregnancy [9, 10].
In suspected cases, either MRI or combined laparoscopy and hysteroscopy can be performed to confirm the diagnosis.
5.1.2 Indications
1.
2.
3.
For patients with asymptomatic rudimentary horn, if ultrasound or MRI confirms that there is uterine endometrium, the rudimentary horn should be prophylactically removed [14].
4.
Whether to remove a rudimentary horn with nonfunctional endometrium is in dispute. Removal of this rudimentary horn does not improve pregnancy outcome.
5.1.3 Timing of Surgery
Depending on the different timing and circumstances when a rudimentary horn is diagnosed, different surgical approaches could be chosen.
For nonpregnancy, it will be practical to perform the resection of rudimentary horn and ipsilateral salpingectomy while the ipsilateral ovary can be preserved. The ipsilateral round ligament and ovary should be suspended over the side of the developed uterus. The location should be opposite to the contralateral round ligament, tube, and ovary of the developed uterus. This is to prevent any torsion of the uterus. With regard to fertility considerations, in patients with abnormalities or absence of the contralateral fallopian tube, there are reports of surgical transplantation of fallopian tube together with its associated uterine horn. For patients with coexistent endometriosis, appropriate surgical treatment should be performed depending on the location of the endometriosis. Patients without fertility issue, radical excision of endometriosis can be performed.
Rupture of the rudimentary horn pregnancy, once diagnosed, should have surgical treatment performed as soon as possible. Patients with acute abdomen and internal bleeding should preferably be explored by laparotomy; if there are no signs of acute internal bleeding or there are stable vital signs, then laparoscopy is acceptable. During early and midtrimester pregnancy, resection of a rudimentary horn and ipsilateral tubal ligation or resection are appropriate to prevent future recurrence of ectopic pregnancy on the side of the rudimentary horn. But the ovary should be preserved and be suspended over the side of the developed uterus. When the pregnancy has reached full term and for those with live births, cesarean section should be performed to save the fetus; the rudimentary horn and ipsilateral fallopian tube should be removed at the same time. Patients without further reproductive demands may consider hysterectomy and bilateral salpingectomy.
5.1.4 Contraindications
Type II A-1c or U5b rudimentary horn is a primordial uterus, while the aplastic uterus has no uterine body and cavity. Whether it is necessary to remove a rudimentary horn with no functional endometrium is still under debate. Also the removal of this type of rudimentary horn does not improve pregnancy outcome.
5.1.5 Preoperative Preparation
1.
Investigation with IVU (intravenous urogram) or MRI is necessary to determine if there is any urinary tract abnormality. If confirmed, a urologist should be consulted for planning a joint operation to avoid multiple surgeries on the same patient. Also, the course and location of the ureters can be determined.
2.
For nonpregnancy surgery, CT angiography may help to determine the blood supply of the rudimentary horn and select the most suitable surgical procedure.
3.
For patients with dysmenorrhea, serum CA125 can be taken to determine the presence of endometriosis.
4.
Preoperative preparations are as for other routine gynecological surgery.
5.
In case of rupture of rudimentary horn pregnancy, blood should be reserved for blood transfusion.
5.1.6 Anesthesia
The patient is placed in a lithotomy position, and general anesthesia with tracheal intubation is performed.
5.1.7 Laparoscopic Resection of Rudimentary Horn
Key surgical techniques [14, 15]:
1.
The round ligament is ligated and cut on the side of the rudimentary horn. The ipsilateral fallopian tube is removed, but the ovary is preserved. When no ovary is found in the pelvis, the descending path of the ovarian development should be explored. Intraoperative ultrasound examination can be used when it is necessary. Keeping detailed records of the ovarian finding is to benefit the patient to seek assisted reproductive technology (ART) for pregnancy.
2.
The ovarian uterine ligament is ligated and cut on the side of the rudimentary horn.
3.
The uterine artery of the rudimentary horn is identified, cut, and controlled by using bipolar coagulation, ultrasonic scalpel, suture, etc. When the uterine artery is to be cut, the position of the ureter must be identified because the vascular supply to the rudimentary horn is directly from the ipsilateral uterine artery, and the ureter may also have shifted higher on the same side.
4.
During removal of the rudimentary horn, care should be taken to avoid removal of too much myometrium of the developed uterus. The hemostasis of the cut raw surface can be controlled by electric coagulation or suture.
5.
After removal of the rudimentary horn, the ipsilateral ovary and round ligament are sutured and suspended onto the side of the developed uterus. The location should be chosen so as to be opposite to the contralateral accessories and round ligament of the developed uterus. This helps to prevent the possibility of torsion of a pregnant uterus in the future.
6.
The resected rudimentary horn can be removed via the pouch of Douglas of the vagina or by an electric morcellator via a trocar in the abdominal wall. Figure 5.3 shows examples of specimens of removed rudimentary uterine horn and ipsilateral fallopian tube.
Fig. 5.3
Specimens of rudimentary horn and ipsilateral fallopian tube removed through the pouch of Douglas from the vagina
7.
At the time of the operation, if the rudimentary horn is found to be distended with retained blood, it can be cut opened to drain the blood; if infection is suspected, blood sample should be taken for bacterial culture and broad-spectrum antibiotics should be given. If careful exploration revealed infection-induced fistula formation between the rudimentary horn and vagina, either laparotomy or laparoscopy combined with vaginal surgery is required to surgically close the fistula [16].
8.
For a patient with coexisting endometriosis, appropriate surgical treatment should be performed according to location of the endometriosis.
5.2 T-Shaped Uterus
Sumin Wang5 and Feng Xu5
(5)
Nanjing Maternity and Infant Hospital of Nanjing Medical University, Nanjing, Jiangsu, P. R. China
Diethylstilbestrol (DES) is a synthetic estrogen which can increase the production of steroid hormone from the placenta during pregnancy, thus reducing the incidence of miscarriages and premature births. It had been widely used from 1948 to 1971 for the treatment for recurrent miscarriages. It was until the relationship of vaginal clear cell carcinoma and the effects of fetal in utero exposure to DES were discovered that its use was then stopped [17]. Early in utero exposure to diethylstilbestrol during pregnancy caused vaginal clear cell carcinoma in only 0.1 % of these patients, while the incidence of the reproductive tract abnormalities occurred in 35–69 % with DES exposure in utero. The uterine abnormality was dose related, and uterine hypoplasia and T-shaped uterine cavity were the most common uterine anomalies. Female fetuses with exposure to DES in utero presented in their adult life with problems of infertility, ectopic pregnancy, spontaneous abortion, and premature delivery [18]. Intrauterine adhesions at lower end of the uterine cavity can also cause uterine narrowing, forming a T-shaped uterine cavity [19].
5.2.1 Diagnosis
According to Buttram and Gibbons (1979) and the American Fertility Society (1988) classification of uterine anomalies, class VII uterine anomalies are related to exposure to DES in utero [20, 21] (Fig. 5.4):
Fig. 5.4
American Fertility Society classification of uterine anomalies – class VII diagrams (Emans SJ, Laufer MR, Goldstein DP. Pediatric and adolescent gynecology. 5th ed. Philadelphia: Lippincott Williams & Wilkins Publishing Company; 2005)
The European Society of Human Reproduction and Embryology (ESHRE) and the European Association of Gynecologic Endoscopy (ESGE) in June 2013 had established a working group under the name of CONUTA (CONgenital UTerine Anomalies) and presented a new consensus ESHRE/ESGE classification system [22]. Type U1 uterine cavity abnormalities (dysmorphic uterus) showed the normal uterine outline but with an abnormal shape of the uterine cavity, usually of small uterine volume. Class 1 is further subdivided into three categories (Fig. 5.5): U1a or T-shaped uterus, characterized by a narrow uterine cavity due to the lateral thickening of the uterine side wall, with a correlation 2/3 uterine corpus and 1/3 cervix; type U1b or uterus infantilis is characterized by a narrow uterine cavity without lateral wall thickening and an inverse correlation of 1/3 uterine body and 2/3 cervix; and type U1c or others, which is added to include all minor uterine cavity abnormalities, such as those with an inner indentation at the fundal midline level of <50 % of the uterine wall thickness. This aims to facilitate groups who want to study patients with minor abnormalities and to clearly differentiate them from patients with septate uterus.
Fig. 5.5
ESHRE/ESGE classification of uterine anomalies of type U1 (Grimbizis et al. [4]). Type U1 is further subdivided into three categories U1a or T-shaped uterus, U1b or uterus infantilis and Type U1c or others. The last one is to include all minor uterine cavity abnormalities
Patients with exposure to DES in utero have reduced fertility and higher incidence of ectopic pregnancy, spontaneous abortion, and premature birth rate than normal women [18, 23]. Their full-term delivery rate in their first pregnancy was 64.1 %, compared to the 84.5 % in those without DES in utero exposure. Further research found that the incidence rates for spontaneous abortion, premature birth, and ectopic pregnancy of women exposed to DES in utero were 19.2 %, 11.5 %, and 4.2 %, respectively, in their first pregnancy, while for those without DES exposure were 10.3 %, 4.1 %, and 0.77 %. Therefore, when the reproductive history of those exposed to DES in utero was analyzed, these patients were more prone to premature birth, early trimester and midtrimester miscarriages, ectopic pregnancy, and so on.
Vaginal ultrasonography can be difficult in detecting DES-related uterine anomalies, while HSG examination is the preferred examination for DES-related uterine anomalies (Fig. 5.6); HSG can define the characteristic T-shaped uterine cavity, with narrow uterine cavity and irregular uterine edge. When combined with a history of exposure to DES in utero, this would lead to a further MRI examination if available to confirm the diagnosis. MRI examination can show the main features of the uterine anomalies caused by DES exposure such as the narrow and irregular uterine cavity, a shorter horizontal uterine segment, and a narrow vertical uterine segment marked by a narrowed band. This band is due to the local thickening of the uterine muscle tissue on both sides. These imaging studies showed the characteristic T-shaped uterine cavity; MRI also can find abnormal cervical development with narrow irregular cervical canal and so on. However, MRI would be difficult to find any tubal abnormality, and it may need saline hydrosonography to assist its diagnosis [24]. HSG and MRI showed a T-shaped uterine cavity, but they still cannot distinguish between various subtypes of T-shaped uterus. Further investigations with hysteroscopy and cervical and endometrial biopsies may be required to confirm the differential diagnosis [25].
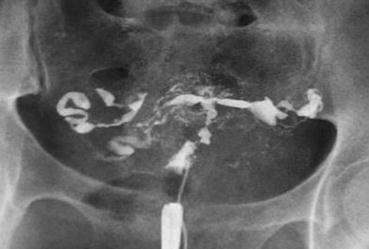
Fig. 5.6
HSG showed the characteristic features of T-shaped, narrow, and irregular uterine cavity
5.2.2 Indications
1.
Unlike other uterine anomalies, a T-shaped uterus due to DES exposure during pregnancy can produce a full-term pregnancy. Therefore, not all patients diagnosed with T-shaped uterus require surgery, but then patients may have a history of adverse pregnancy outcome such as spontaneous miscarriage, premature birth, etc., and after excluding other causes of miscarriage, hysteroscopic corrective surgery is the appropriate treatment.
2.
Intrauterine adhesions can also cause T-shaped uterus. If the narrow uterine cavity and endometrial damage lead to scanty menstruation, miscarriage, and other adverse pregnancy outcomes, hysteroscopic surgery may be required.
3.
Patients with DES exposure in utero might have cervical incompetence due to abnormal uterine and cervical anomalies. During pregnancy, bed rest and preventive or emergency cervical cerclage might be needed to avoid midtrimester miscarriage and premature birth. Therefore, it had been suggested that in DES-exposed pregnant women, prophylactic cervical cerclage should be performed during pregnancy. However, prophylactic cervical cerclage during pregnancy is still controversial, and further RCT studies will be needed [18, 26].
5.2.3 Timing of Surgery
Hysteroscopic surgery should be offered to patients with T-shaped uterine cavity and a history of infertility or adverse pregnancy outcomes. It can also be used to treat patients who failed IVF-ET treatment. Surgery can be performed soon after menstruation to avoid a thickened endometrium which might impact on the hysteroscopic surgery.
5.2.4 Contraindications
1.
It is important to exclude other factors leading to infertility, recurrent miscarriage, and premature labor. Then hysteroscopic surgery can be chosen to treat this uterine factor that is responsible for the adverse pregnancy outcomes. Otherwise, treatments should be directed to treat other relevant factors.
2.
Patients with adhesion-induced T-shaped uterus, particularly those aged over 40 years of age, require a comprehensive assessment of their reproductive potential. Only after effective communication with patients should surgery be performed; otherwise, in patients without fertility issue or with no significant menstrual changes, there is no need for any surgery. Combined estrogen and progesterone therapy would be given if it is necessary.
3.
Patients with T-shaped uterine cavity due to exposure to DES in utero do not require surgery if they have no history of adverse pregnancy outcome.
5.2.5 Preoperative Preparation
1.
According to HSG or 3D ultrasound findings, the measurements of the distance between tubal openings, the depth of uterine cavity, and the bilateral and fundal myometrium thickness would give an assessment of the amount and depth of uterine wall excision during surgery.
2.
Oral contraceptives can be used to control the endometrial thickness 1 month before the surgery.
3.
Routine preoperative preparations are as other gynecological surgery. Twelve to twenty-four hours before the surgery, softening of the cervix by insertion of a laminaria tent might be useful as cervical preoperative treatment in some patients.
5.2.6 Anesthesia
Intravenous anesthesia or general anesthesia can be chosen. Patients should have vital signs and electrolytes monitoring so as to avoid the fluid overload “TURP” syndrome.
5.2.7 T-Shaped Uterine Cavity Surgery
Key surgical techniques for T-shaped uterine cavity hysteroscopic surgery [19, 27–29]:
1.




Intraoperative ultrasound monitoring to increase the safety of the surgery.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
