Chapter 2 ABNORMAL PREMENOPAUSAL UTERINE BLEEDING
In women of childbearing age, abnormal uterine bleeding includes any change in menstrual period frequency, duration, or amount of flow, as well as bleeding between cycles. A menstrual cycle of fewer than 21 days or more than 35 days is considered abnormal. Likewise, a menstrual flow of fewer than 2 days or more than 7 days is abnormal.
When abnormal uterine bleeding is evaluated (Figs. 2-1 and 2-2), it is important to make certain that the bleeding is not from a gastrointestinal or urinary source. Once it is clear that the bleeding is vaginal, pregnancy should be the first consideration in women of childbearing age. After pregnancy has been ruled out, iatrogenic causes of abnormal uterine bleeding should be considered. Medications linked to abnormal premenopausal uterine bleeding are outlined later in this chapter. After pregnancy and iatrogenic causes have been excluded, systemic conditions should be considered. These systemic causes and the suggested workup, outlined later in the chapter, include thyroid, hematologic, pituitary, hepatic, adrenal, and hypothalamic disorders.

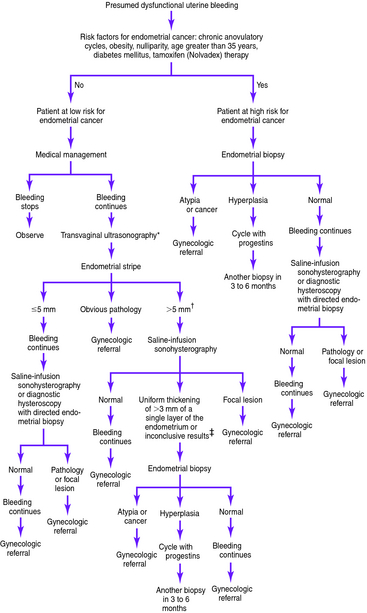
Figure 2-2. Presumed dysfunctional uterine bleeding in women of childbearing age: evaluation based on risk factors for endometrial cancer.*†‡
Of cases of endometrial carcinoma, 20% to 25% occur before menopause, and the risk of developing endometrial cancer increases with age. Thus, the American College of Obstetricians and Gynecologists recommends endometrial evaluation in women aged 35 and older who have abnormal uterine bleeding. Endometrial evaluation is also recommended for patients younger than 35 who are at high risk for endometrial cancer. Women with vaginal bleeding who are younger than 35 years and have no identifiable risk factors for neoplasia can be assumed to have dysfunctional bleeding and treated accordingly. However, if bleeding continues in a patient at low risk for neoplasia despite medical management, endometrial evaluation is indicated.



