421. Friends are considering adopting a “special needs” child from another country. The family has few details, but the video provided by the Bombay, India adoption agency of the 4-year-old child shows an adorable, healthy-appearing, active, blue-eyed boy. The child does not speak much on the video, rather lapses into gibberish sounds, and does not seem to follow directions from the social worker very well. You are suspicious this child may have which of the following syndromes?
a. Kleinfelter
b. Waardenberg
c. Marfan
d. Down
e. Turner
422. A 13-year-old asymptomatic girl is shown below. She states that the findings demonstrated began more than a year ago. Which of the following is the most likely diagnosis?
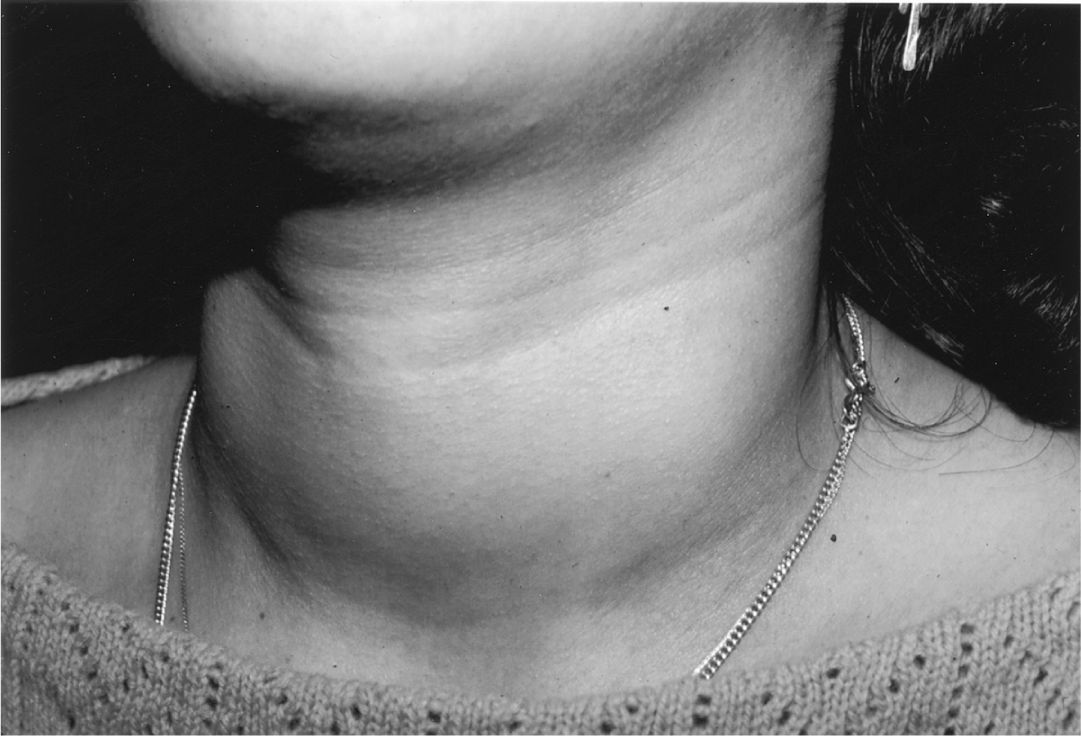
(Courtesy of Adelaide Hebert, MD.)
a. Iodine deficiency
b. Congenital hypothyroidism
c. Graves disease
d. Exogenous ingestion of Synthroid
e. Lymphocytic (Hashimoto) thyroiditis
423. During a routine well-child examination, a 12-year-old girl reports that she has occasional headache, “racing heart,” abdominal pain, and dizziness. Her mother states that she has witnessed one of the episodes, which occurred during an outing at the mall, and reported the child to be pale and to have sweating as well. Other than some hypertension, she has a normal physical examination. Which of the following is an appropriate next step in the evaluation and management of this child?
a. Breath into a paper sack should the symptoms return
b. Measurement of serum β-HCG levels
c. Determination of HbA1C levels
d. Measurement of urine vanillylmandelic acid (VMA) and homovanillic acid (HVA) and serum metanephrine levels
e. MRI of the brain
424. The 10-year-old child shown weighs 55 kg (> 99 percentile; 50 percentile for a 14 year old), has central fat distribution, is 125-cm tall (5 percentile), has a blood pressure of 120/80 mm Hg, a hematocrit of 17%, and her bone films are read as “osteopenic.” Which of the following disorders is most likely responsible for the clinical picture that this boy presents?

a. Bilateral adrenal hyperplasia
b. Adrenal adenoma
c. Adrenal carcinoma
d. Craniopharyngioma
e. Ectopic adrenocorticotropin-producing tumor
425. A 6-year-old boy is brought to your practice by his paternal grandmother for his first visit. She has recently received custody of him after his mother entered the penal system in another state; she does not have much information about him. You note that the child is short for his age, has downslanting palpebral fissures, ptosis, low-set and malformed ears, a broad and webbed neck, shield chest, and cryptorchidism. You hear a systolic ejection murmur in the pulmonic region. His grandmother reports that he does well in regular classes, but has been diagnosed with learning disabilities and receives speech therapy for language delay. His constellation of symptoms is suggestive of which of the following?
a. Noonan syndrome
b. Congenital hypothyroidism
c. Turner syndrome
d. Congenital rubella
e. Down syndrome
426. The parents of a 2-week-old infant bring him to the emergency center in your local hospital for emesis and listlessness. Both of his parents wanted a natural birth, so he was born at home and has not yet been to see a physician. On examination, you find a dehydrated, listless, and irritable infant. Although you do not have a birth weight, the parents do not feel that he has gained much weight. He has significant jaundice. His abdominal examination is significant for both hepatomegaly and splenomegaly. Laboratory values include a total bilirubin of 15.8 mg/dL and a direct bilirubin of 5.5 mg/dL. His liver function tests are elevated and his serum glucose is 38 mg/dL. His admit urinalysis is negative for glucose but positive for Gram-negative rods; his urine and his blood ultimately grow E coll. Which of the following nutritional considerations should be considered in this child?
a. Administration of high doses of vitamin B6
b. Initial diet free of branched-chain amino acids
c. Lactose free formula
d. Protein restriction and supplementation with citrulline
e. Initiation of a diet low or free of phenylalanine
427. You see in consultation a 2-year-old child from a local institution for chronically ill children. He was born normal but had significant developmental delay noted in the first months of life. Early in his life he had significant vomiting and was once evaluated for pyloric stenosis although the testing for this was negative. He is now hyperactive, and has much purposeless movements with rhythmic rocking and athetosis noted. The family notes that his only other illnesses have been mild seborrhea and eczema, which have got better over time. As you compare him to his 2 older siblings in the room, you note that his skin is of lighter color. You note a distinctive, unpleasant “mousy” smell in the room. Which of the following testing results is likely to explain this child’s condition?
a. Elevated quantitative fecal fat levels
b. Elevated levels of blood or urine succinylacetone
c. Finding of high blood levels of methionine and homocystine
d. Elevated serum phenylalanine levels
e. Finding on plasma amino acid analysis elevations of leucine, isoleucine, valine, and alloisoleucine and depression of alanine
428. An otherwise healthy 7-year-old child is brought to you to be evaluated because he is the shortest child in his class. Careful measurements of his upper and lower body segments demonstrate normal body proportions for his age. Which of the following disorders of growth should remain in your differential?
a. Achondroplasia
b. Morquio disease
c. Hypothyroidism
d. Growth hormone deficiency
e. Marfan syndrome
429. The state laboratory calls your office telling you that a newborn infant, now 8 days old, has an elevated thyroid stimulating hormone (TSH) and low thyroxin (T4) on his newborn screen. If this condition is left untreated, the infant is likely to demonstrate which of the following in the first few months of life?
a. Hyperreflexia
b. Hyperirritability
c. Diarrhea
d. Prolonged jaundice
e. Hyperphagia
430. A 1-year-old boy presents with the complaint from his parents of “not developing normally.” He was the product of an uneventful term pregnancy and delivery, and reportedly was normal at birth. His previous healthcare provider noted his developmental delay, and also noted that the child seemed to have an enlarged spleen and liver. On your examination, you confirm the developmental delay and the hepatosplenomegaly, and also notice that the child has short stature, macrocephaly, hirsutism, a coarse facies, and decreased joint mobility. Which of the following is the most likely etiology of his condition?
a. Beckwith-Wiedemann syndrome
b. Crouzon syndrome
c. Trisomy 18 (Edwards syndrome)
d. Jeune syndrome
e. Hurler syndrome
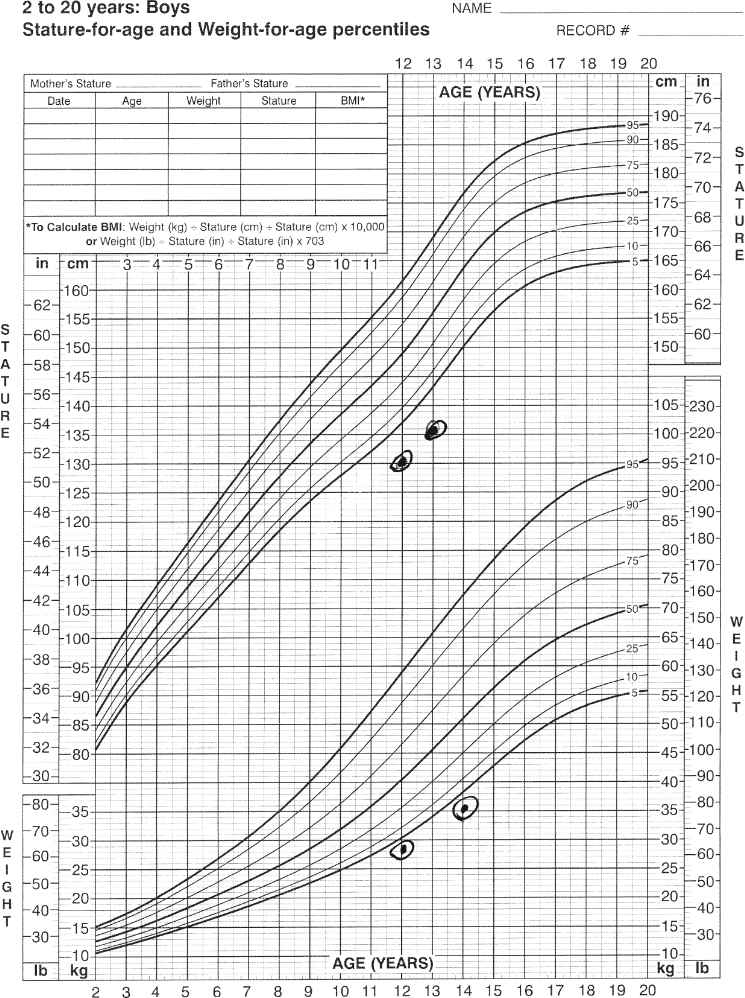
431. A 13-year-old boy comes to your office expressing concern about his height. He had first seen you a year prior for his routine check-up and a preparticipation sports physical for soccer (see growth curve). Now in the eighth grade, all of his friends are taller than he is, and he is at a disadvantage on the soccer field playing against much larger boys. After obtaining height information from his parents shown here, you order a skeletal bone age radiograph. Which of the following results would allow you to assure him of an excellent prognosis for normal adult height?
a. A bone age of 9 years
b. A bone age of 13 years
c. A bone age of 15 years
d. Being at the 50th percentile for weight
e. Being at the 3rd percentile for weight
432. In counseling the parents of the child pictured, which of the following statements is true?
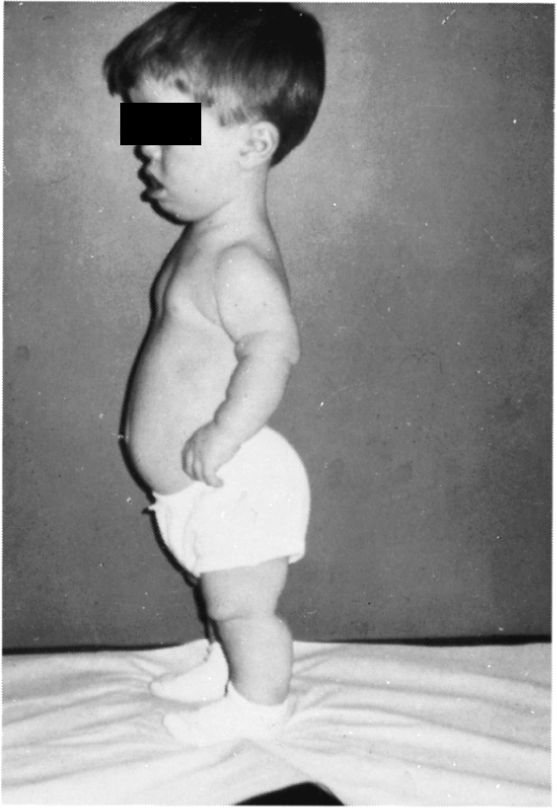
a. Delayed motor milestones is likely
b. Normal intelligence is expected
c. Infertility is a likely outcome
d. Ventriculoperitoneal shunting for hydrocephalus will likely be required
e. Ultimate normal height and weight is expected
433. A 12-year-old girl has a solitary thyroid nodule found on routine examination; she has no symptoms. Which of the following is the most appropriate next step for this patient?
a. Fine needle aspirate
b. CT scan of the neck
c. Serum thyroid function tests
d. Trial of suppressive T4 treatment to look for nodule shrinkage
e. Excisional biopsy
434. The 16-month-old male infant pictured below was recently brought from a developing country to the United States. The family history reveals that his father had an eye and a leg removed. Which of the following is the most likely diagnosis?

(Courtesy of Kathryn Musgrove, MD.)
a. Coloboma of the choroid
b. Retinal detachment
c. Nematode endophthalmitis
d. Retinoblastoma
e. Persistent hyperplastic primary vitreous
435. A 4-year-old child has mental retardation, shortness of stature, brachydactyly (especially of the fourth and fifth digits), and obesity with round facies and short neck. The child is followed by an ophthalmologist for subcapsular cataracts, and has previously been noted to have cutaneous and subcutaneous calcifications, as well as perivascular calcifications of the basal ganglia. This patient is most likely to have which of the following features?
a. Hypercalcemia
b. Hypophosphatemia
c. Elevated concentrations of parathyroid hormone
d. Advanced height age
e. Decreased bone density, particularly in the skull
436. A 15-year-old boy has been immobilized in a double hip spica cast for 6 weeks after having fractured his femur in a skiing accident. He has become depressed and listless during the past few days and has complained of nausea and constipation. He is found to have microscopic hematuria and a blood pressure of 150/100 mm Hg. Which of the following is the most appropriate course of action?
a. Request a psychiatric evaluation.
b. Check blood pressure every 2 hours for 2 days.
c. Collect urine for measurement of the calcium to creatinine ratio.
d. Order a renal sonogram and intravenous pyelogram (IVP).
e. Measure 24-hour urinary protein.
437. An adolescent with type 1 diabetes returns for a follow-up visit after his annual check-up last week. You note that his serum glucose is elevated, and his glycosylated hemoglobin (hemoglobin A1C) is 16.7%. This finding suggests poor control of his diabetes over at least which of the following time periods?
a. 8 hours
b. 1 week
c. 1 month
d. 2 months
e. 6 months
438. A 7-day-old boy is admitted to a hospital for evaluation of vomiting and dehydration. This is the third child for this family, and the prenatal history was uncomplicated. Physical examination on the child is normal except for some hyperpigmentation of the nipples. Serum sodium and potassium concentrations are 120 mEq/L and 9 mEq/L (without hemolysis), respectively; serum glucose is 35 mg/dL. Which of the following testing is most likely to result in this child’s diagnosis?
a. Ultrasound of the pylorus
b. Measure of his 17-hydroxyprogrosterone level
c. Measurement of his T3, T4, and TSH levels
d. MRI of the pituitary
e. Chemical analysis of the commercial formula being fed to the child
439. A 14-year-old boy presents with the complaint of “breast swelling.” The boy reports that he has been in good health and without other problems, but has noticed over the past month or so that his left breast has been “achy” and that he has now noticed some mild swelling under the nipple. He has never seen discharge; the other breast has not been swelling; and he denies trauma. Your examination demonstrates a quarter-sized area of breast tissue under the left nipple that is not tender and has no discharge. The right breast has no such tissue. He has a normal genitourinary examination, and is Tanner stage 3. Which of the following is the best next course of action?
a. CT scan of the pituitary
b. Measurement of serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH)
c. Measurement of serum testosterone
d. Reassurance of the normalcy of the condition
e. Chromosomes
440. An infant is brought to a hospital because her wet diapers turn black when they are exposed to air. Physical examination is normal. Urine is positive both for reducing substance and when tested with ferric chloride. This disorder is caused by a deficiency of which of the following?
a. Homogentisic acid oxidase
b. Phenylalanine hydroxylase
c. L-histidine ammonialyase
d. Ketoacid decarboxylase
e. Isovaleryl-CoA dehydrogenase
441. An 18-year-old girl has hepatosplenomegaly, an intention tremor, dysarthria, dystonia, and deterioration in her school performance. She also developed abnormal urine with excess glucose, protein, and uric acid. She has a several-year history of elevated liver enzymes of unknown etiology. Which of the following best explains her condition?
a. Indian childhood cirrhosis
b. α1-Antitrypsin deficiency
c. Menkes syndrome
d. Dubin-Johnson syndrome
e. Wilson disease
442. A 3-month-old infant without significant past history was brought to the emergency center by her mother with a generalized tonic-clonic seizure. She is found to have glucose of 5 mg/dL. After correction of her hypoglycemia, she is admitted to your service for further evaluation. Several hours later, her nurse calls to tell you that her bedside glucose check was now 10 mg/dL. You order laboratory work suggested by the pediatric endocrinology team and again correct the infant’s hypoglycemia. The results of the laboratory tests you drew include an elevated serum insulin level of 50 μU/mL, and a low IGFBP-1 (plasma insulin-like growth factor binding protein-1). C-peptide levels are not detectable. Which of the following is the likely cause of this child’s recurrent hypoglycemia?
a. Nesidioblastosis
b. Pancreatitis
c. Beckwith-Wiedemann syndrome
d. Galactosemia
e. Factitious hypoglycemia
443. An 11-year-old boy is the tallest child in his sixth grade class. He is thin, has a high arched palate, mild scoliosis, and joint hyperextensibility. He is an honor student, and enjoys basketball but must use prescription sports goggles, so he can see the ball on the court. He is likely to have which of the following conditions?
a. Cerebral gigantism (Sotos syndrome)
b. Homocystinuria
c. XXY (Klinefelter syndrome)
d. Marfan syndrome
e. XYY
444. A very upset mother brings her 8-month-old child to the emergency room because he will not move his leg. She reports that when she was carrying him to the car about half an hour ago, she slipped on some ice and fell on top of him. The mother, an 18-year-old African American woman, has been exclusively breast-feeding her child. She has only recently started him on cereals, and has not supplemented his diet with vitamins. A radiograph of the child’s leg is shown below. Which of the following laboratory findings would be expected?

(Courtesy of Susan John, MD.)
a. Hypocalcemia
b. Hypophosphaturia
c. Reduced serum alkaline phosphatase
d. Hypocalciuria
e. Hyperphosphatemia
445. A small-for-gestational-age infant is born at 30 weeks’ gestation. At 1 hour of age, his serum glucose is noted to be 20 mg/dL (normally greater than 40 mg/dL). Which of the following is the most likely explanation for hypoglycemia in this infant?
a. Inadequate stores of nutrients
b. Adrenal immaturity
c. Pituitary immaturity
d. Insulin excess
e. Glucagon deficiency
446. A 1-day-old normal-appearing infant develops tetany and convulsions. He was born at 34 weeks’ gestation with Apgar scores of 2 and 4 (at 1 and 5 minutes, respectively) to a woman whose pregnancy was complicated by diabetes mellitus and pregnancy-induced hypertension. Which of the following serum chemistry values is likely to be the explanation for his condition?
a. Serum bicarbonate level of 22 mEq/dL
b. Serum calcium of 6.2 mg/dL
c. Serum glucose of 45 mg/dL
d. Serum magnesium level of 5.0 mg/dL
e. Intracranial hemorrhage
Questions 447 to 451
For each of the disorders listed below, select the serum concentration of calcium (Ca2+) and phosphate (PO4) with which it is most likely to be associated. Each lettered option may be used once, more than once, or not at all.
a. Low PO4, normal Ca
b. Low PO4, high Ca
c. Normal PO4, low Ca
d. Normal PO4, normal Ca
e. High PO4, low Ca
447. Three boys in a family with hypodense calcification of their bones and a history of fractures; their condition is unresponsive to dietary changes or vitamin supplementation
448. A short, 4-year-old, mentally retarded child with brachydactyly of the fourth and fifth digits; obesity with round facies; short neck; subcapsular cataracts; and cutaneous, subcutaneous, and perivascular calcifications of the basal ganglia
449. A 4-year-old child with blue sclera and a history of multiple fractures with minimal trauma
450. A 6-year-old child who complains of numbness and tingling of the hands, and later develops tonic-clonic seizures
451. An otherwise healthy 18-year-old girl with medullary thyroid carcinoma
Questions 452 to 457
All the syndromes listed below are associated with overweight conditions in children. For each of the other clinical findings that follow, select the syndrome with which it is most likely to be associated. Each lettered option may be used once, more than once, or not at all.
a. Prader-Willi syndrome
b. Laurence-Moon-Biedl syndrome
c. Cushing syndrome
d. Fröhlich syndrome
e. Pseudohypoparathyroidism
f. Polycystic ovary syndrome
g. Type 2 diabetes
452. A 15-year-old defensive lineman for his high school football team whose mother reports that his shoulder pads have permanently stained his neck
453. A 6-day-old infant with severe hypotonia and poor feeding since birth
454. A 5-year-old boy with mental retardation and polydactyly
455. A 5-day-old girl with brachydactyly, round facies, and short neck
456. A 15-year-old girl with menstrual irregularities and hirsutism
457. A 14-year-old boy with hypogonadism and night blindness with retinitis pigmentosa
Questions 458 to 463
For each of the following disorders, select the serum concentrations (mEq/L) of sodium (Na+) and potassium (K+) with which it is most likely to be associated in a dehydrated patient. Each lettered option may be used once, more than once, or not at all.
a. Na+118, K+7.5
b. Na+125, K+3.0
c. Na+ 134, K+ 6.0
d. Na+ 144, K+ 2.9
e. Na+155, K+ 5.5
458. A 3-week-old baby presents to the emergency room with a history of poor feeding, vomiting, weight loss, and decreased urine output. You recognize immediately the name of the child as you have been trying without success to reach the family as their son’s newborn metabolic screen returned suspicious for 21-hydroxylase deficiency (adrenogenital syndrome).
459. An 11-year-old boy has been involved in an automobile accident. During his recovery in the intensive care unit he is noted to have large amounts of what appears to be dilute urine output.
460. A 1-year-old girl has recently moved into your area. The family members who bring her to see you have no paperwork and they seem to be developmentally delayed. You can glean from them that the girl, like several other family members, urinates a great deal, has had multiple hospitalizations for dehydration, and her previous doctors have told the family to “make sure she gets plenty to drink.”
461. A 4-year-old boy is noted to have blood pressure measurements about 30 mm Hg higher than normal but appears to be otherwise fine. Upon close evaluation of the family history, you find that many in his family have had early-onset hypertension and several have had strokes. In addition to abnormal electrolytes, this child also has elevated serum levels of aldosterone but low plasma renin activity.
462. An 8-year-old boy has a diagnosis of Addison disease. However, he is on vacation at his grandmother’s house when he is involved in an automobile crash and sustains a fractured femur; his grandmother is intubated in the surgical intensive care unit. While his family is arriving from out of state, he develops a number of electrolyte abnormalities.
463. A 1-year-old girl has had since about 3 months of age repeated episodes of hypoglycemic seizures and bouts of lactacidosis. She has a protuberant abdomen due to her massive hepatomegaly, a doll-like facies, thin extremities, and is short for her age. Upon drawing her blood, you are struck by the “milky” appearance.
Questions 464 to 470
Patients with genetic disorders, or those affected by specific teratogens in utero, typically have certain characteristic dysmorphic features. Match the physical description with the genetic or teratogenic abnormality. Each lettered option may be used once, more than once, or not at all.
a. Trisomy 21 (Down syndrome)
b. Trisomy 18 (Edwards syndrome)
c. Holt-Oram syndrome
d. Diabetic embryopathy
e. Fetal alcohol syndrome
f. Turner syndrome
g. Ehlers-Danlos syndrome
464. A 10-year-old boy with hypermobile joints and poor wound healing.
465. A 6-year-old girl with cognitive delay, a blowing systolic heart murmur, short stature, round face, bilateral transpalmar crease, upslanting palpebral fissures, small ears, and epicanthal folds.
466. A newborn has low sloping shoulders, right hand attached at elbow with agenesis of the forearm, cardiac abnormalities, missing chest wall musculature, and a bifid thumb.
467. A 2-year-old boy, less than the 5% for weight and height, is in early childhood intervention for developmental delay. He has a short nose, thin upper lip with thin vermillion border, a ventricular septal defect (VSD), and short palpebral fissures.
468. A 14-year-old girl with short stature, thick neck, minimal pubertal development, repaired coarctation of the aorta, and normal intelligence.
469. A small newborn with a large VSD, clenched hands, cleft palate, rounded heels, and a horseshoe kidney.
470. A newborn with hypoglycemia, hypocalcemia, and hypoplastic lower extremities.
Questions 471 to 474
New discoveries made possible by advances in molecular genetics have broadened our understanding of nontraditional inheritance. Match the disease and the mode of inheritance to the clinical scenario provided. Each lettered option may be used once, more than once, or not at all.
a. MELAS (mitochondrial inheritance)
b. Hypomelanosis of Ito (mosaicism)
c. Prader-Willi syndrome (genomic imprinting)
d. Turner syndrome (sex chromosome imbalance)
e. Huntington chorea (triplet repeat expansion disorder)
471. A 3-year-old boy has gradually developed delayed motor and cognitive delays as well as short stature. He has had several episodes of strokelike episodes, lactic acidosis, seizures, and recurrent severe headaches. He has cytochrome oxidase-negative ragged red fibers noted on muscle biopsy.
472. A mentally retarded 4-year-old boy who was noted to be hypotonic at birth and had failure to thrive in infancy now has a tremendous appetite, obesity, hypogonadism, and small hands and feet
473. A previously normal father of one of your patients develops ataxia and tremor. Many other members of the family have mental retardation; the men are notable for having long facies, large ears, micropenis, and large testes.
474. A developmentally delayed 2-year-old child has seizures, microcephaly, and hypotonia as well as bilateral hypopigmented whorls on the upper extremities.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


