BILIARY TRACT
What is the most likely diagnosis?
a. Biliary colic
b. Cholecystitis
c. Choledocholithiasis
d. Cholangitis
e. Pancreatitis
Answer a. Biliary colic
Right upper quadrant pain that radiates to the right scapula in a “fat, fertile, forty female” is always caused by gallstones. Symptoms of gallstones are almost always postprandial because a rise in cholecystokinin (CCK) causes the gallbladder to contract and cause partial obstruction of the cystic duct, causing bile egress to be disrupted. This causes sharp pain that last about 30 minutes, coincidently, the same amount of time CCK is present. Cholecystitis would present with RUQ pain and fevers, and choledocholithiasis are stones in the common bile duct (CBD); CBD presents with jaundice. Cholangitis presents with fevers, RUQ, and jaundice, and pancreatitis is the classic epigastric pain radiating into the back.
The largest component of gallstones is cholesterol. Calcium bilirubin and pigment are additives.
Fat + Fertile + Forty + Female = Estrogen
Estrogen = Smooth muscle relaxant = Causes biliary stasis = Gallstones
What is the best diagnostic test?
a. Computed tomography (CT) scan of the abdomen
b. Abdominal ultrasonography
c. Endoscopic retrograde cholangiopancreatography (ERCP)
d. Magnetic resonance imaging (MRI) of the abdomen
Answer b. Abdominal ultrasonography
Abdominal ultrasonography is the best initial test and most accurate test. Findings of gallstones include acoustic shadowing, which means there are no sound waves seen below the stone or posterior to it. Ultrasonography has greater sensitivity and specificity than CT scan. ERCP is used to both diagnose and remove stones in the complete blood count (CBC) but is not used in imaging of the gallbladder. MRI of the abdomen is always the wrong answer for abdominal processes.
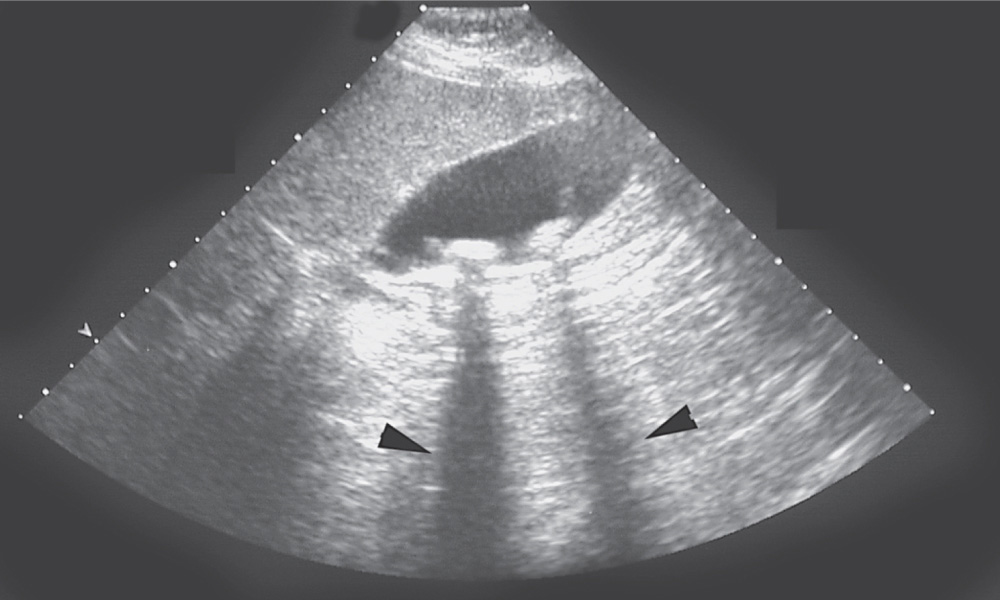
Figure 10-1. Ultrasonography showing two echogenic gallstones in the gallbladder. Note the absence of echoes posterior to the gallstone called “shadowing” (arrowheads). (Reproduced, with permission, from Brunicardi FC, et al. Schwartz’s Principles of Surgery. 10th ed. New York: McGraw-Hill; 2015.)
What is the best next step in the management of this patient?
a. Laparoscopic cholecystectomy
b. Open cholecystectomy
c. Antibiotic treatment
d. Ursodeoxycholic acid
Answer a. Laparoscopic cholecystectomy
The most appropriate therapy for a patient with symptomatic gallstones is laparoscopic cholecystectomy. Asymptomatic gallstones can be managed expectantly. Open cholecystectomy is the correct answer for patients with ruptured cholecystitis. Antibiotic therapy is the best initial therapy for acute cholecystectomy and would not help this patient because of the lack of infection. Medical treatment with ursodeoxycholic acid is never the correct answer and is only used in patients who are poor surgical candidates or have very small stones (<1 cm).
What is the most likely diagnosis?
a. Peptic ulcer disease
b. Cholecystitis
c. Choledocholithiasis
d. Pancreatitis
Answer b. Cholecystitis
The findings of RUQ pain, fever, and Murphy’s sign are indicative of cholecystitis. Cholecystitis is caused by blockage of the cystic duct that leads to distension of the gallbladder and subsequent surrounding inflammation caused by bacterial overgrowth. The pain starts in the epigastric region and then localizes to the RUQ. Peptic ulcer disease does have epigastric pain, but the pain increases with eating, not after eating. Pancreatitis is constant epigastric pain that radiates to the back but would not have a positive Murphy’s sign.
The cystic duct merges with the common hepatic duct to form the common bile duct (Figure 10-2).
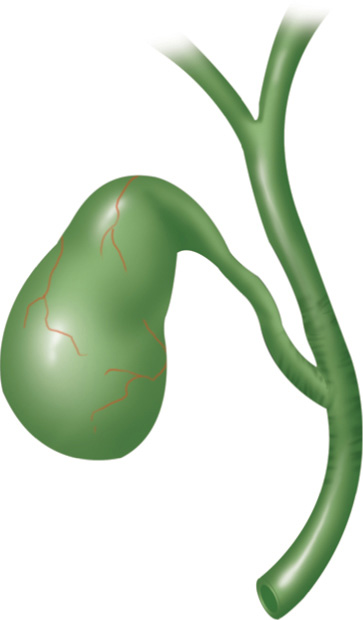
Figure 10-2. Junction between the cystic duct and common hepatic duct. (Reproduced, with permission, from Brunicardi F, Andersen DK, Billiar TR, et al, eds. Schwartz’s Principles of Surgery. 9th ed. New York: McGraw-Hill; 2010.)
What is the best next step in the management of this patient?
a. Complete blood count (CBC)
b. Comprehensive metabolic profile (CMP)
c. Normal saline
d. Intravenous (IV) access
e. Nothing by mouth (NPO)
f. All of the above
Answer f. All of the above
Upon realization that the patient has an infectious process in the abdomen, laboratory evidence of an inflammatory process and IV fluids are the best next steps.
What is the best initial test to confirm your diagnosis?
a. CT scan of the abdomen
b. Abdominal ultrasonography
c. Endoscopic retrograde cholangiopancreatography (ERCP)
d. Magnetic resonance imaging (MRI) of the abdomen
e. Hepatobiliary scintigraphy (HIDA)
Answer b. Abdominal ultrasonography
Ultrasonography is 95% sensitive and 80% specific for cholecystitis. The sonographic features of acute cholecystitis include gallbladder wall thickening (>5 mm), pericholecystic fluid, gallbladder distention (>5 cm), and a sonographic Murphy’s sign.
HIDA scan is the most accurate test for acute cholecystitis but is only used when the diagnosis is equivocal on ultrasonography. A finding that is pathognomonic for acute cholecystitis on HIDA is “nonvisualization of the gallbladder” (Figure 10-3).
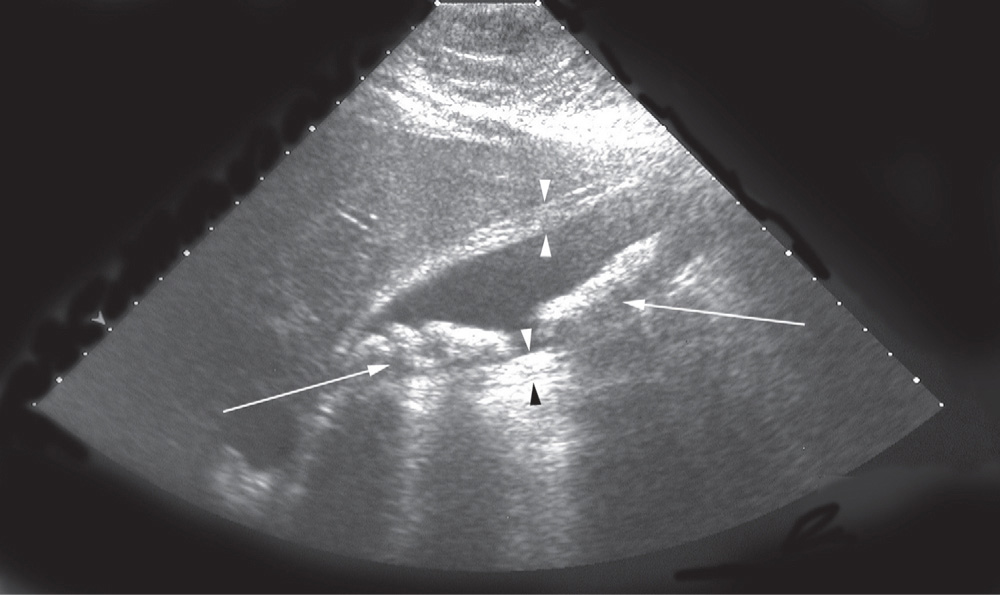
Figure 10-3. Ultrasonography from a patient with acute cholecystitis. The arrowheads indicate the thickened gallbladder wall. There are several stones in the gallbladder (arrows) throwing acoustic shadows. (Reproduced, with permission, from Brunicardi F, Andersen DK, Billiar TR, et al, eds. Schwartz’s Principles of Surgery. 9th ed. New York: McGraw-Hill; 2010.)
Orders:
• Abdominal ultrasonography
• Ciprofloxacin
• Metronidazole
Ultrasonography reveals a gallbladder wall thickness of 7mm, pericholecystic fluid, gallbladder distention of 6 cm, and numerous gallstones (Figure 10-4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


